|
Abstract:
This study
aims to evaluate the efficacy of flexible intramedullary (IM)
nails as a fixation device of paediatric femoral shaft
fractures. A total of 11 children with 11closed fractures were
treated by this method. The patients ranged in age from 6 to 12
years and the mean follow-up was 18 weeks. All patients had open
femoral growth plates at the time of surgery. All fractures
united and none of the patients needed re-operation.
No major complications were recorded. After nail removal, all
children had full range of hip and knee motion. At final
follow-up, none of the children presented with clinical
malalignment of the fractured limb. Maximum angulation that was
calculated on the coronal plane was 5° into varus and on the
sagittal plane 7°of anterior angulation (apex posteriorly).
Leg-length discrepancy was assessed clinically and
radiographically when needed.A Flexible nailing of diaphyseal
fractures of the femur is a reliable method with a small
learning curve and allows early mobilisation. Most of our minor
complications were technique related and could be avoided1
J.Orthopaedics 2010;7(3)e6
Keywords:
Flexible nails; Femoral fractures; Childhood
Introduction:
Paediatric femoral fractures are treated by a variety of methods
including traction, immediate spica cast, traction followed by
spica cast, internal fixation with plate and screws, external
fixation and intramedullary fixation. Orthopaedic surgeons
remain divided about the optimal method of treatment for
children's femoral fractures. The choice of treatment may be
influenced by the age of the child, the level and pattern of the
fracture and to a great extent, by regional, institutional or
surgeons' preferences
2.
A systematic review of the literature provides little evidence
to support one method of treatment over another3.
In general, outcomes tend to be uniformly good irrespective of
the method of treatment.
Inclusion Criteria:
Age 6 to 12 years, open femoral physes; closed midshaft femur
fracture; no concomitant injuries to either lower extremity; no
history of injury to either femur; no history of asymmetric
femoral malalignment; agree to participate in 18 weeks of follow
up; informed consent1
Exclusion Criteria:
open midshaft femur fractures; other injuries to either lower
extremity; a history of injury to either femur; unable to comply
with 2 years of follow-up1
Elastic Stable Intramedullary Nailing
The technique of elastic stable intramedullary nailing, adapted
from existing flexible rod systems, was first described by
surgeons from Nancy, France4,5. Ligier et al reported
the results of the Nancy experience5. The technique
has become one of the most popular methods of fixation of
paediatric femoral fractures in North America1. Excellent
clinical results have been reported with this technique, which
has been variously called "elastic stable intramedullary
nailing", "flexible intramedullary nailing" or "Nancy nailing"6-9.
Perceived advantages of this technique include earlier
mobilization and more rapid return to function than with
nonoperative techniques, and less soft tissue disruption and
smaller scars when compared with other surgical methods5.

Fig 1. Mid diaphyseal fracture
Principle of "Elastic Stability"
The flexible rod is initially bent or curved (plastically
deformed). During intramedullary insertion, which is typically
retrograde in the femur, the relatively straight medullary canal
(compared with the contoured nail) forces the curved rod to
straighten within the bone. This elastic deformation creates a
bending moment within the long bone which will tend to angulate
the fracture in the direction and the plane of the concavity of
the curved rod, as the rod wants to return to its initial curved
state. This moment is counteracted by a second rod of matched
diameter and curve, which balances the first rod with an equal
but opposite moment. The two intramedullary nails act
complimentarily to stabilize the fracture. This biologic
fixation is not rigid but sufficiently stable against angular,
translational and torsional deforming forces and is associated
with early formation of exuberant callus. Typically , no
additional external immobilization is required. However, any
significant imbalance in the magnitude or the direction of the
moment created by the two nails will result in angulation of the
fracture in the direction of the stronger nail.
The titanium nails have been distinguished from other flexible
nail systems such as Ender nails, made of stainless steel. The
latter are believed to be insufficiently elastic for children's
fractures6.
Sometimes three or more flexible rods are inserted in order to
better fill the medullary canal to enhance cortical contact, and
provide more stable fixation. This constitutes a form of rigid
intramedullary fixation, quite different from the Nancy nailing
concept.
 
Fig 2. Proximal Long Spiral fracture
Indications
Elastic stable intramedullary nailing is ideally suited for mid-diaphyseal
transverse, short oblique or short spiral fractures of the femur
with minimal comminution, in children 6 to 12 years old who are
being considered for operative stabilization (Fig. 1). The use
of flexible nails can be extended to more proximal, even
subtrochanteric fractures and some multifragmentary fractures by
modifying the technique to take advantage of the principles
outlined above (Fig. 2). The addition of external protection
like a knee immobilizer can limit the overall motion of the
lower extremity and reduce the deforming forces on the fracture
in these situations10.
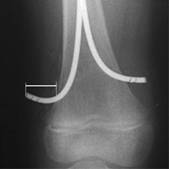 
Fig 3: Do not leave nail tips bent or prominent.
Fig: 4
Countering of nail at C-shaped configuration with apex at the
fracture site
Fig: 5
Nail diameter should not exceed 40% diameter of narrowest
part of medullary cavity
Materials
and Methods:
The
material of this study consisted of 11 children with 11femoral
shaft fractures treated by titanium elastic nail fixation at
department of Orthopaedics, B.P.Koirala institute of health
sciences, Dharan, Nepal. The age incidence in this series ranged
from 6 years to 12 years (an average of 9 years),. 7 children
(63.6%) were males and 5 (45.4%) were females. All the fractures
in this series were recent closed fractures. The fracture
pattern was transverse or short oblique in 9 cases and
comminuted in two cases. All the fractures occupied the middle
third of the femur.. The mechanism of injury included pedestrian
vehicle accidents (60%), motor vehicle accidents (28%) and falls
(12%). There were no associated injuries in this series. All the
fractures in this series were treated by retrograde titanium
elastic nail fixation using two nails of equal diameter for each
fracture. The surgical technique was as follows: Under general
anaesthesia, the child was positioned supine on a fracture table
with a traction boot and traction was applied to the injured
extremity followed by adjustment of the image intensifier
(C-arm) for obtaining anteroposterior and lateral views for the
injured femur intraoperatively. The nail diameter was determined
on preoperative radiographs (Fig. 1). After sterilisation and
draping of the injured extremity, the planned entry point for
the nails were checked using image intensifier( 2-3 cm above
distal femoral physis) then two TENS of equal diameter were
inserted after proper countering and advance proximally to
fracture site. Fracture were reduced closed and nails were
advanced proximally one after another.
 
Fig:6
Pre-operative Photograph
 
Fig:7
Post-Operative photograph
Throughout
the procedure, position of nails were checked by image and
finally distal ends of nails were cut sothat they can flush into
the femoral condyles. Any distraction at the fracture was
checked and if any corrected by releasing traction.Out of 15
cases, two cases required open reduction. the nail diameter used
in this series were 3mm in 10 cases, 2.5mm in 3 cases and 2mm in
2cases.Wound was closed and Above Knee POP slab was applied in
all cases for 2 weeks i.e till suture removal. The patients was
put on non weight bearing axillary crutch walking. The patients
were followed up clinico-radiologically and look for fracture
healing upto 3 months to sixy months.
Results :
The hospital stay ranged between 3 to 15 days, there was no post
operative infection . All fractures united in 8 weeks to 12
weeks time. There were limb length discrepancy in 5 cases which
is less than 2 cm. There was no angulational and rotational
deformity. there was no implant failure as well as migration of
implant.In 2 cases there were irritation of skin at the implat
insertion site. Implant was removed an average of 6 months(5-7
months). There were no voilation of cortex either medial or
lateral in this series.The most common complications reported in
this series are pain and skin irritation at the entry site
associated with the prominence of the ends of the nails9. Nail
ends should not be bent, as was originally recommended, but
advanced so that they lie against the supracondylar flare of the
femur in order to avoid symptoms at the insertion site. Use of
nails of two different diameters is associated with a high rate
of loss of reduction in the direction of the stronger rod9.
Multifragmentary fractures might be better stabilized by
alternative methods of fixation. If used in comminuted
fractures, these should be monitored weekly for early loss of
reduction, and they might benefit from some additional external
immobilization
Although the originators of this technique recommended routine
removal of the nails, there is no evidence that this is
necessary in the absence of nail-related symptoms.
Discussion :
Paediatric femoral fractures are treated by a variety of methods
including traction, immediate spica cast, traction followed by
spica cast, internal fixation with plate and screws, external
fixation and intramedullary fixation1.
The indications for TENS for fixation of paediatric femoral
shaft fractures are expanding as their advantages are realized
and complications of other operative methods of stabilization
are reported. Compression platings are associated with high
incidence of refracture. External fixators are associated with
pin tract infection, loss of reduction, refracture vafter
removal of external fixator. rigid intramedullary nailing are
associated with greater trochanter physis leading to growth
arrest with subsequent coxa valga. It is also associated with
damage to blood supply of femoral head leading to osteonecrosis
of femoral head.These problems and complications are overcome by
introduction of flexible intramedullary nailing(TENS) for
treatment of paediatric femoral shaft fractures with following
advantages2-3
·
Price are comparable and are available in different diameter
·
inserted without voilation of growth plate
·
Excellent purchase of nails in the bone due to dense medullary
cavity of immature skeletal
·
Removal of nails are not associated withrefracture as they are
load-sharing device
Our results are compatible with results of other series of TENS
in terms of union, no implant failur,no refracture after implant
removal, within acceptable limb length descrepancies
Summary
Elastic stable intramedullary nailing is an excellent method of
managing most, but not all, paediatric femoral fractures that
need operative stabilization1. It is by no
means the only technique nor is there evidence yet that it is
superior to other methods. Its advantages make it a valuable
choice to consider in managing these fractures. Ultimately, the
choice should reflect best evidence and also incorporate patient
preferences2
Reference:
- John A, Dimitios P, Charalampos K, Kristos P, George M., et
al. Flexible intramedullary nailing in paediatric femoral
shaft fractures. Clinical trials Volume 41, Issue 6, Pages
578-582
- Sanders J.O., Browne R.H., Mooney J.F., et al.
Treatment of femoral fractures in children by pediatric
orthopedists: Results of a 1998 survey.
J Pediatr Orthop 2001;21:436-441.
- Wright J.G.
The treatment of femoral shaft fractures in children: A
systematic overview and critical appraisal of the literature.
Can J Surg /J Chir Can 2000;43:180-189.
- Ligier J.N., Metaizeau J.P., Prévot J.
Closed flexible medulary nailing in pediatric traumatology.
Chir Pediatr 1983;24(6):383-5.
- Metaizeau J.P.
L'osteosynthese chez l'enfant par embrochage centro medullaire
elastique stable.
Sauramps Medical, Montpellier 1988.
- Ligier J.N., Metaizeau J.P., Prévot J.,
Lascombes P. Elastic stable intramedullary nailing of femoral
shaft fractures in children.
J Bone Joint Surg [Br] 1988;70-B:74-7.
- Bar-On E., Sagiv S., Porat S.
External fixation or flexible intramedullary nailing for
femoral shaft fractures in children.
J Bone Joint Surg. [Br] 1997;79-B: 975-8.
- Flynn J.M., Hresko T., Reynolds R.A.K., Blasier R.D., et al..
Titanium Elastic nails for Pediatric Femur fractures: A
multicenter study of early results with analysis of
complications.
J Pediatr Orthop 2001;21:4-8.
- Carey T.P., Galpin R.D.
Flexible intramedullary nail fixation of pediatric femoral
fractures.
Clin Orthop 1996;332:110-118.
- Narayanan U.G., Hyman J.E., Wainwright A.M., Rang M., Alman
B.A.
The complications of elastic stable intramedullary nail
fixation of paediatric femoral fractures, and how to avoid
them. 2002.
Submitted to J Pediatr Orthop.
|

