|
Huang Gang-yong, Wei Yi-bing , Xia Jun ,Wu
Jian-guo, Chen Fei-yan, Chen Jie, Wang Si-qun.
Department of Orthopeadics, Huashan Hospital, Fudan University,
Shanghai, 200040, China
Address for Correspondence:
Xia Jun
Department of Orthopeadics, Huashan Hospital, Fudan University,
No.12, Wulumuqi Road(Middle), Shanghai, 200040, China
E-mail:
cormierhuang@yahoo.com.cn
|
|
Abstract:
Objective To compare the patellar tracking with pheumatic
tourniquet inflated on straight leg and maximally flexed knees.
Merterials and Methods 20 inpatients normal knees with
consents were enrolled to the study. The Caton Index and
trochlear angle were recorded at 30°flexion
of the knees under general aneasthesia without tourniquet. We
inflated the pheumatic thigh tourniquets on straight leg and
maximally flexed knees as contrast groups, and the Laurin angle
and Merchant congruent angle were recorded at 30°,45°,60°,90°and
120°knee
flexion at sunrise view. These angles were compared to describe
different patellar tracking. Results At 30°flexion,
Caton Index averaged 1.02±0.19 and trochlear angle was 138.9±7.4°.
The Merchant congruent angle tends to be larger during knee
flexing with most significant changes as the knee flexed from 30°to
45°. The
Laurin angle presented no significant change at the whole range
of knee flexion. The Merchant congruent angle and Laurin angle
of patellofemoral joint show no significant difference with
pheumatic tourniquet inflated on either straight leg or
maximally flexed knees. Conclusion For normal knees, the
main kinematic effect of pheumatic tourniquet on the
patellofemoral joint with different knee flexion are presented
at the initial 45°flexion
of knee which is observed as increasement of Merchant congruent
angle, while Laurin angle keeps no significant change during the
whole range of motion. The patellar tracking shows no
significant difference with pheumatic tourniquet inflated on
either straight leg or maximally flexed knees.
J.Orthopaedics 2009;6(3)e3
Keywords:
patellofemoral joint; Kinematics; Pheumatic tourniquet
Introduction:
The pneumatic tourniquet is widely used in knee surgery. It
guarantees less blood loss and easier exposure of the surgical
fields. On the other hand, the tourniquet restricts the smooth
movement of the quadriceps, which might in turn change
patellofemoral kinematics theoretically. It has been justified
in total knee arthroplasties.1 The emphasis
should be attached to the patellofemoral congruency especially
when doing the kinematic changing operations such as dealing
with knee arthroplasty and patellofemoral instability. Could the
modification of pneumatic tourniquet fixation and inflation
diminish its influence on patellar tracking? This study aimed to
compare the patellofemoral congruency values with pheumatic
tourniquet secured and inflated on straight leg and maximally
flexed knees in normal individuals.
Materials
and Methods:
With approval of the ethical review board and consents of the
patients, the study recuited 20 inhospital patients from the
Orthopedics Ward without knee disorders or anterior knee pain
complaints, whose age ranged from 18 to 45 years. There were 14
male cases and 6 female cases. The study was done when the
patient undergone operation of the other skeletal structures
except the knees under general anesthesia. Only one randomized
knee of each patient was selected to undergo the study to
protect the attendees from excessive X-ray exposure.
Firstly, the Caton Index2 and trochlear angle were
recorded at 30°flexion
of knees. Then we set the pheumatic tourniquet at 120°
flexed knees and inflated to 60Kpa on maximally flexed position
(Group I), and the Laurin angle(figure
1)3
and the Merchant congruent angle(figure
2)4
were recorded at 30°,45°,60°,90°and
120°knee
sunrise view. Ten minutes rest after these manipulations, the
tourniquet was secured and inflated to 60Kpa at the same knee
which was extensed fully (Group II ) and the Laurin Angle and
the Merchant congruent angle were measured at different knee
flexion as abovementioned. These angles were measured by two
independent orthopaedic surgeons and the averaged values were
used for analysis. These angles were compared to describe
different patellar tracking. We used the Sirimobil Iso-C X-ray
intensifier (Simens, Germany) to record the images. Paired
samples t test was adopted to analyse the Laurin angle and
Merchant congruency angle differences between flexed and
extensed knee groups . One sample t test was adopted to analyse
the changes of the Laurin angle and Merchant congruency angle
among different degrees of knee flexion at each group. P<0.05
was considered statistically significant level.
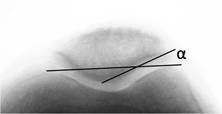
Figure 1 Laurin angle

Figure 2 Merchant congruency angle
Results :
At the knees of 30°flexion,
Caton Index averaged 1.02±0.19 and trochlear angle was 138.9±7.4°.
The Merchant congruent angle tended to be larger during knee
flexing, with most significant changes as the knee flexed from
30°to 45°.
The Laurin angle presented no significant change at the whole
range of knee flexion. The Merchant congruent angle and Laurin
angle of patellofemoral joint show no significant difference
with pheumatic tourniquet secured and inflated on either
straight leg or maximally flexed knees.(table 1)
|
Knee flexion
(degrees)
|
trochlear angle
(degrees±sd) |
Laurin angle
(degrees±sd) |
Merchant angle
(degrees±sd) |
|
Group I |
Group II |
Group I |
Group II |
|
30° |
138.9±7.4° |
21. 6±5.5 |
21.4±4.9 |
-5.2±5.1 |
-5.4±4.9 |
|
45°
|
138.5±7.9 |
20.4±4.2 |
20.8±5.3 |
-10.5±4.4 |
-10.2±5.2 |
|
60° |
137.8±8.9 |
19.9±4.5 |
20.2±5.4 |
-10.2±3.7 |
-10.1±4.6 |
|
90° |
137.1±9.1 |
21.5±4.7 |
21.0±4.9 |
-12.3±5.4 |
-12.0±5.1 |
|
120° |
137.6±10.3 |
24.5±5.1 |
24.3±5.2 |
-10.3±5.8 |
-10.5±5.5 |
Table 1 Patellar tracking changes when flexing knees
Discussion :
The patellar tracking are mandatorily assessed by surgeons both
in TKA and in intervention of patellofemoral disorders. Due to
high tension of quadriceps by tourniquet inflation, No Thumb
Test in the TKA operation may mislead to lateral tilt of
patella. The same situation also appears in other
patellofemoral management. 5,6,7
To our knowledge, the patella is seated in suprapatellar bursa
as the knee fully extenses. And it slides into femoral trochlear
groove by the pull of medial vastus femoris and medial
patellofemoral ligament as knee flexion reaches 15°to
20°. The
patella is stabilized in deeper trochlear groove as knee flexion
is larger than 70°and
less chance is that instability or subluxation of patella
occurs. Sunrise or Merchant view of patella at 20
°to 30°flexion
of knee is vital to evaluate the development of trochlear and
stability of patellofemoral joint . Most of knee X-ray indexes
are assessed at this position, and the trochlear angle and Caton
index of patella height are also measured at the same position.
Insall-Salvati index is widely used to evaluate the height of
patella. In this study Caton index is used instead of
Insall-Salvati index considering we always pay close attention
to joint line level in joint surgery. The Laurin angle and
Merchant congruency angle are used to see the stability at
different knee flexion angles in this study. When we assess the
patellar tilt the line connecting posterior condyles of femur is
reliable and in most cases considered as one of the best
references. The line connection the anterior condyles are always
less reliable due to various development of distal femur. Based
on the fact that we would put the patients under radiation
exposure of CT if we measured patellar tilt with posterior
condylar reference, the Laurin angle was chosen in this study .
Additionally, the comparation of Laurin angle of those
patients same knees eliminated the adverse influence by
anatomical varieties. The Merchant congruency angle can be
accessible in various flexion of knee to assess the
lateralization of patella and it keeps good application of
clinical relevance. 2,3
The results showed patellar height with 1.02±0.19 of Caton index
and trochlear groove development with 138.9±7.4°of
trochlear groove angle. These are similar to the results of
established knowledge , and it indicates application of ordinary
population. The arcuated contour of trochlear brought difficulty
to measurement and may exaggerate errors. It is known that
patellar tilt will be more obvious when the tension of
quadriceps of femoris are increased by tourniquet after
the VMO and medial retinaculum have been recised. The
performance of Laurin angle in this study indicates patella tilt
has not been infuenced by different tourniquet fixation groups
when retinacular structures were intact . The changes of
Merchant congruency angle at the initial 45°flexion
of knee in this study may caused by the process of patellar
slide from suprapatellar bursa to trochlear groove. While in
deep flexion of knee, the Merchant congruency angle presented no
significant further change under any alteration of quadriceps
tension.
With incised medial retinaculum the pneumatic tourniquet
increases the tilt of patella so that inflation of tourniquet at
maximally flexed knee has the potential advantage of less
interference of quadriceps femoris which protects from patellar
tracking changes. 6,7
As a major result of this study, the Merchant congruent angle
and Laurin angle of patellofemoral joint show no significant
difference with pheumatic tourniquet inflated at either extensed
or flexed knees. This should be interpreted as that with intact
medial retinaculum the patellofemoral congruency does not change
significantly caused by different position of pneumatic
tourniquet.
This study has the potential advantage of reliability as an
own-control study in vivo and objective indexes observed. To
protect the enrolled cases from escessive exposure under
radiation of X-ray we chose randomly one side of knee and we use
C-arm auto-protection system of Siemens to guarantee the safety.
Because the Laurin angle and Merchant congruency angle was not
obtained in a continuous style and the three dimensional data
can not be reached, it is only a preliminary attemptation to
understand the kinematics of patellofemoral joint and further
investigation can be done in a three dimensional pattern.
Reference :
-
Thorey
F, Colsman CS, Windhagen H, et al. The
effect of tourniquet release timing on perioperative blood
loss in simultaneous bilateral cemented total knee
arthroplasty: a prospective randomized study. Technol
Health Care. 2008;16(2):85-92.
-
Caton J, Deschamps G, Chambat P, et al. Les rotules
basses: A propos de 128 observations. Rev Chir Orthop.
1982;68:317-25.
-
Laurin CA, Dussault R, Levesque HP. The tangential x-ray
investigation of the patellofemoral joint: X-ray technique,
diagnostic criteria and their interpretation. Clin Orthop.
1979;144:16-26.
-
Merchant AC, Mercer RL, Jacobsen RH, et al. Roentgenogrphic
analysis of patella-femoral congruence. J Bone Joint Surg.
1974;56A:1391-6.
-
Fu FH, Maday MG. Arthroscopic lateral release and the lateral
patellar compression syndrome. Orthop Clin North Am.
1992;23:601-12.
-
Marson BM,
Tokish JT. The effect of a tourniquet on intraoperative
patellofemoral tracking during total knee arthroplasty.
J Arthroplasty. 1999;14:197-9.
-
Husted H, Toftgaard JT. Influence of the Pneumatic Tourniquet
on Patella Tracking in Total Knee Arthroplasty: A Prospective
Randomized Study in 100 Patients. J Arthroplasty.
2005;20(6):694 7.
|

