| ORIGINAL
ARTICLE |
|
New Promising Brace for Clubfoot
Management-A new unilateral dynamic custom-made brace used after
Ponseti manipulation for idiopathic congenital talipes equinovarus
deformity. |
|
El-Sayed MH*, Correll J**, Pholig K***
*
Consultant of Pediatric Orthopedics, Egypt.
**Correll J, Chief of Staff and Director of Aschau Specialized
Pediatric Orthopedic Hospital, Germany.
***Pholig K, Pohlig GmbH, Traunstein, Germany.
Address for Correspondence:
El-Sayed MH*,
MD. PhD.
Lecturer & Consultant of Pediatric Orthopedics,
Tanta University Hospital, Egypt.
Consultant of Pediatric Orthopedics,
96, Hasan Radwan St., Dr.Mostafa Hosni Building,
Tanta, Gharbia, Egypt. P.O.Box 3111,
Fax: +2 040 3315916,
Tel: +2 010 663 26 28.
E-mail:
mhosney2001@hotmail.com
|
|
Abstract:
There are
many, commercially available, braces present for the after-care
of patients with clubfoot deformity, with the Dennis Browne
splints being the most commonly used ones. The boots used with
this type of orthosis are mounted on transverse bars, to hold
the foot in abduction. These braces fix both feet together
although in most the cases the condition is unilateral.
Moreover, they are some times accompanied by psychological
stigmata, which might lead to interruption of treatment and is
followed by recurrence of the deformity.
The
reported unsatisfactory results, especially because of the
parents non-compliance, gave way to the appearance of
knee-ankle-foot braces. They alternatively provided unilateral
foot stabilization at the required position of correction.
Unfortunately, some models fixed the knee in about 90 degrees of
flexion with subsequent motion restriction, disuse atrophy of
the gatrocnemius muscle, and Achilles tendon shortening.
We have
developed a new dynamic custom-made brace, which does not only
allow for free movement of the healthy side in unilateral cases,
but also full range of motion of the hip and knee joints, and a
controllable range of active movement of the ankle joint of the
affected side.
This new
brace allows graded and controlled active dorsi-flexion and
plantar-flexion of the ankle joint, and appears to have better
family compliance.
J.Orthopaedics 2008;5(3)e10
Keywords:
Clubfoot;
Ponseti; Denis Browne; new brace; orthosis.
Introduction:
Congenital
talipes equinovarus deformity (clubfoot), is probably the most
common congenital orthopedic condition requiring intensive
treatment. It represents a congenital dysplasia of all the
musculoskeletal tissues distal to the knee (1). This deformity
consists of intraosseous components (within the bones), as well
as interosseous components (resulting from abnormal bony
relationships). This deformity affects mainly the tarsus, with
the tarsal bones, which are mostly made of cartilage, are in the
most extreme position of flexion, adduction, and inversion at
birth (2).
Nowadays,
there is almost universal agreement that the initial management
of idiopathic clubfeet should be non-operative, regardless of
the severity of the deformity. This entails serial gentle
manipulations followed by long-leg cast application at weekly
intervals (3-7). Many authors have emphasized on the importance
of early management, and it is now settled that the earlier the
treatment is begun, the more likely that it would be successful
(8-10).
Failure of
the conservative management, including the Ponseti method, has
been frequently attributed to the non-compliance with the use of
the orthosis after correction has been obtained (11-14). This
was usually attributed to the long time use of the brace (
ranged 2 to 4 years), psychological problems and fear of some
parents from appearance in public with their child wearing the
brace, and the thought that it would be a stigma for their
children in their future lives. Moreover, the Denis Browne had
the disadvantage of holding both feet, this in turn limit the
hip and knee movements of the healthy sides well. For all the
above mentioned reasons, we have developed a unilateral brace
that should hold the affected side only in the desired position
after correction, in order to avoid any parents discomfort from
the voluminous transverse bar, to allow normal free movements of
the healthy side, and to allow controlled motion of the affected
side as well.
Kinematics
and Biomechanics of the Brace
According
to Ponseti, correction of clubfoot deformity is accomplished by
abducting the foot in supination while counter-pressure is
applied over the lateral aspect of the head of the talus bone,
to prevent rotation of the talus in the ankle. After a achieving
full correction with or without percutaneous Achilles tendon
tenotomy, the brace is used to maintain the position of
correction of the foot. The regular braces depended on the bar
connection between both legs to gain the abduction needed for
the forefoot. Foot abduction is required is required to
maintain the abduction of the calcaneus and forefoot to prevent
recurrence, while the knee joints are left free bilaterally, so
that the child would extend his knees (kicking movement). In
addition, this movement is crucial for active stretching of the
gatrocnemius muscles, and the Achilles tendon. The new brace
holds the femoral condyles to control foot abduction, but leaves
the anterior and posterior aspects of the knee free to allow for
complete range of knee motion in the sagittal plane. Thats how,
the brace controls the thigh-foot axis and the lateral rotation
of the foot at the desired angle of correction ( about 70
degrees). At the level of the ankle joint, the brace is modified
to allow for gradual dorsal extension and plantar flexion as
required during successive phases of management. The applied
protocol at Aschau Hospital was to restrict any ankle movement
(lock the joint), during the first three months (full-time
period). Afterwards, active ankle motion was permitted (unlock
the joint) through specially designed joints mounted along the
mechanical axis of movement of the ankle, medially and
laterally. The whole foot was stabilized in abduction, while
lateral pressure was applied against the head of the talus
(three points of correction). The degree of foot supination was
also controllable. Plain X-ray film in the lateral view was done
routinely, to assure the position of correction. In contrary to
the Denis Browne brace, which was insufficient to hold the heel
in place and to prevent it from sliding up and down into the
boots, the new brace was perfectly moulded around the foot and
allowed no heel displacement during application. This was also
confirmed with the lateral X-ray film done.

Fig.1:The
new brace; anterior view: note how the brace controls the angle
of foot abduction and supination, holds firmly the knee from the
sides, allow free knee joint movement, have joints at the level
of the ankle joint to allow for controlled ankle motion.

Fig.2 :
Lateral
view of the brace; note the hinges mounted on the brace on both
sides at the ankle joint to allow gradual active controlled foot
movement.
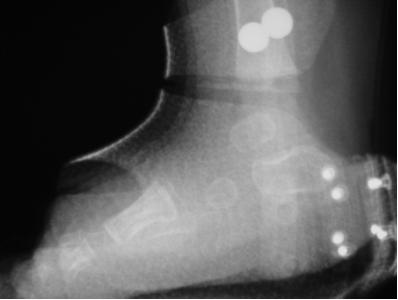
Fig.3:
Lateral
view radiograph of the foot within the brace, to check the
position of the foot, to make sure that the brace fits the foot
adequately and to check the position of the hinges in relation
to the ankle joint.
Discussion :
Noncompliance associated with the use of different types of
splints, after correction of clubfeet, was considered as one of
the most common causes for recurrence of the deformity.
Although, many authors have reported full deformity correction
after successive manipulations and casting, the risk of
recurrence due to family noncompliance was always high. The
parents usually complained form the bulky appearance and the
long duration of application of the orthosis. We have developed
a new unilateral brace to avoid the bulky brace in unilateral
cases and to avoid using the connection bar in bilateral ones.
The new brace perfectly controls the thigh-foot axis (degree of
external rotation), allows active controlled ankle motion, and
spares the movement of the ipsilateral knee and hip. The brace
was found acceptable and tolerable by the parents. The
short-term initial results show better compliance rates. No
complications were reported with the use of this brace. We think
it is a good alternative to the original Denis Browne brace
specially in unilateral clubfoot cases.
Reference :
1.
Herring JA. Tachdjians pediatric orthopedics. Vol.3. W.
B. Saunders company, 2002: 922-59.
2.
Herzenberg JE, Carroll NC, Christofersen MR, et al.
Clubfoot
analysis with the three dimensional computer modeling. JPO 1988:
8-257.
3.
Ponseti IV. Congenital clubfoot: Fundamentals of
treatment. Oxford, Oxford University Press 1996.
4.
Kite JH. Nonoperative treatment of congenital clubfoot.
Clin Orthop 1972: 84; 29-38.
5.
Cowell HR. The management of clubfoot. JBJS (Am) 1985:
67; 991-2.
6.
Ponseti IV, Smoley EN. Congenital clubfoot: the results
of treatment. JBJS (Am) 1963: 45; 261-75.
7.
Mckay DW. New concept and approach to clubfoot treatment:
section II- Correction of clubfoot. JPO 1983: 3; 10-21.
8.
Seringe R, Atia R. Idiopathic congenital talipes
equino-varus: The results of manipulative treatment (269 feet).
French J Orthop Surg. 1990: 4; 342.
9.
Crawford AH, Gupta AK. Clubfoot controversies:
complications and causes of failure. Inst Course Lect. 1996: 45;
339-46.
10.
Yamamoto H, Muneta T, Morita S. Nonsurgical treatment of
congenital clubfoot with manipulation, cast, and ,modified Denis
Browne splint. JPO 1998: 18; 538-42.
11.
Hutchins PM, Foster BK, Paterson DC, Cole EA. Long term
results of early surgical release in club feet. JBJS (Br) 1982:
67; 791-9.
12.
Arnson J, Puskarich CL. Diformity and disability from
treated clubfoot. JPO 1990: 10; 109-19.
13.
Roye DP Jr, Roye BD. Idiopathic congenital talipes
equinovarus. JAAOS 2002: 10; 239-48.
14.
Dobbs MB, Rudzki JR, Purcell DB, et al. Factors
predictive of outcome after use of the Ponseti method for
treatment of idiopathic Clubfeet. JBJS ( Am) 2004: 86; 22-7.
|
|
This is a peer reviewed paper Please cite as
:
El-Sayed
MH : New
Promising Brace for Clubfoot Management-A new unilateral dynamic
custom-made brace used after Ponseti manipulation for idiopathic
congenital talipes equinovarus deformity.
J.Orthopaedics 2008;5(3)e10
URL:
http://www.jortho.org/2008/5/3/e10 |
|
|

