|
Abstract:
Bursitis
with rice bodies is a rare disease that can appear as a
complication of a chronic bursitis. Although
it was initially described as being related to tuberculosis, it
is currently more often associated with inflammatory
arthropathies, such as rheumatoid arthritis (RA). It is
important to make an early diagnosis, since the removal of rice
bodies causes symptom resolution and prevents process
perpetuation. By
using magnetic resonance imaging (MRI) combined with plain
radiographs (X-ray) and ultrasound, it is possible to make a
correct preoperative diagnosis.
We
present a new case of subacromial-subdeltoid bursitis with rice
bodies as a first manifestation of previously undiagnosed RA.
J.Orthopaedics 2007;4(4)e24
Keywords:
Bursitis;
Magnetic Resonance Imaging,
Arthritis,Rheumatoid, Shoulder Joint, ultrasonography,
Diagnostic Imaging
Introduction:
Bursitis
with rice bodies is a rare disease that can appear as a
complication of subacromial-subdeltoid bursitis. Bursitis with
rice bodies was first described in tuberculosis arthritis by
Riese in 1896. However, it is currently more often associated
with inflammatory arthropathies, such as rheumatoid arthritis.
It may also occur in the absence of systemic disease.
Plain
X-ray is often
normal, showing at times an unspecified increase of soft
tissues. Calcified nodes are not observed in the plain X-ray.
The
ultrasound scan shows fluid in the bursa with multiple
hyperechogenic nodular images.
The
MRI shows multiple hypointense nodes in all sequences.
The low signal intensity in the T2-weighted sequences is a
characteristic finding that makes it possible to restrict the
diagnosis and rule out other diagnoses with high intensity
signal in such sequences, such as synovial lipomatosis and
synovial proliferation.
Synovial
chondromatosis usually appears with visible calcifications in
the X ray in the late phases. In the non-mineralized phases
nodes have a high intensity signal in the T2-weighted sequences.
Although they can
show a low signal intensity, this intensity is always observed
with a signal gap in the gradient echo sequences, which does not
occur in bursitis with rice bodies. The presence of fluid inside
the bursa with multiple hypointense nodules in all the sequences
in the absence of calcifications in the plain X- ray must
immediately suggest the diagnosis of bursitis with rice bodies
and lead to an early surgery that avoids symptom perpetuation
and process worsening.
Case Report:
Fifty-three-year-old
woman with a history of pain in her right shoulder for 8 months,
with an increase of the deltoid volume, which has progressed in
the last two months. The
patient has no history of prior shoulder injury.
Physical
examination highlights an evident right shoulder volume
increase, with the aspect of a subdeltoid mass. No active or
passive movement limitation (ROM) is seen. Preoperative Constant
score (Table 1) was reduced, due mainly to pain. Passive
mobilization of the humeral head provoked a crepitation on the
deltoid mass.
Rheumatoid
factor (RF) and antinuclear antibodies were negative. Elevated
C-reactive protein and a high erythrocyte sedimentation rate (54
mg/L and
30 mm
, respectively) were the only positive data in the laboratory
analytical results.
Plain
X rays showed increased soft tissues in the right shoulder, with
no evidence of calcifications.
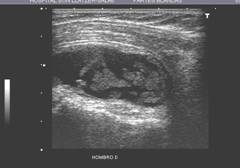
Ultrasound
(Fig. 1) showed subacromial-subdeltoid and subcoracoid bursas
distension due to the presence of multiple hyperechogenic oval
nodules with uniform size within the bursa.
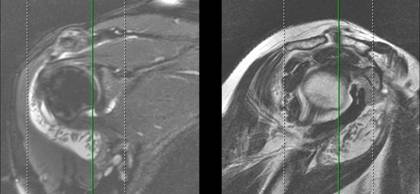
MRI
(Fig. 2) showed significant amounts of fluid in the
subacromial-subdeltoid and subcoracoid bursas, with multiple
oval nodules with hypointense signal intensity in all the
sequences. Findings were coherent with bursitis with rice
bodies. Arthroscopic approach of the subacromial space showed a
very thickened subacromial bursa, which was erroneously
interpreted as the rotator cuff, and prevented the observation
of rice bodies in the arthroscopic exploration. No arthroscopic
intra-articular exploration was carried out, to avoid the spread
of disease in case it was secondary to tuberculosis. Open
debridement was carried out in the same surgical procedure, via
a deltopectoral approach (Fig. 3). A very thickened bursa
containing multiple rice bodies was found (Figs. 3 and 4).
Findings
were confirmed by means of pathological examination.
Immediately
following surgery, the patient exhibited complete resolution of
all symptoms in the shoulder.
Then
the patient presented with pain and swelling in the right ankle.
Imaging techniques showed massive joint effusion and sinovial
proliferation. Rheumatoid arthritis was suspected, and the
patient was referred to the Rheumatology Department, where a
methotrexate treatment was initiated, frankly resolving the
symptoms. Currently, the patient is asymptomatic.
Discussion :
Bursitis with rice bodies was first described by Riese in 1896
in tuberculosis arthritis(1). It is currently more frequent in
chronic inflammatory arthritis, such as RA.
Rice bodies consist of a heterogeneous group of particles that
may contain collagen, fibrinogen, fibrin, fibronectin,
mononuclear cells, blood cells and amorphous material. The cause
of rice bodies formation is not fully clear. De novo rice bodies
formation has been suggested by some authors. Some other authors
have suggested that rice bodies are produced secondary to
micro-infarcts in the hypertrophied sinovial capsule. In the
present case, the existence of similar symptoms in the ankle,
which showed a significant sinovial proliferation, could suggest
this last theory and lead to the possibility of finding an early
phase of rice bodies formation. In any case, it seems evident
that rice bodies could be considered as an irritant factor in a
hypertrophic sinovial capsule, and that its existence could lead
to a vicious cycle in which the inflammatory process is
perpetuated. This hypothesis is supported by the fact that rice
bodies elimination will eliminate symptoms in the involved
joint.
Plain X-ray is usually normal, even though a non-specific
increase of rice bodies may be seen. Typically, no
calcifications are seen.
Few references are found in the literature about the diagnosis
of bursitis with rice bodies by means of ultrasound, even though
this must be the first-choice technique in the presence of any
soft tissues mass non-suggestive of malignancy. Multiple
hyperechogenic homogeneous images of uniform size with a bursa
full of fluid were found in ultrasound. The lack of posterior
acoustic shadow allows for ruling out the diagnosis of
mineralized sinovial chondromatosis. Based on ultrasound,
differential diagnosis with sinovial lipomatosis and sinovial
proliferation should be made, which are easily ruled out by
means of MRI, due to the high signal intensity in T2-weighted
sequences in these two conditions(2).
MRI shows multiple low-density nodules in all the sequences. The
presence of low signal intensity in T2-weighted sequences, along
with the lack of calcifications in the plain X-ray and lack of
signal gap in GRE sequences must immediately suggest the
diagnosis of bursitis with rice bodies(2).
Management of bursitis with rice bodies depends on the cause. In
the case of bursitis with rice bodies secondary to rheumatoid
arthritis, the most adequate management seems to be the
elimination of rice bodies, combined with systemic treatment for
the disease.
In the present case, no macroscopic leak was observed between
the bursal content and the gleno-humeral joint. As in other
reported cases(3), no evidence of rotator cuff tear was found.
Even though the gleno-humeral joint showed joint effusion, no
rice bodies were found within the joint. It seems that this
unusual presentation of RA spares the gleno-humeral joint, which
contrasts with the evident bursal involvement(4-7).
Conclusion:
The
presence of a distended bursa with multiple hypointense signal
intensity nodules in all the MRI sequences, not associated
with plain X-ray calcifications and signal gap in T2-weighted
sequences, must indicate the diagnosis of bursitis with rice
bodies and lead to an early surgical procedure in order to
avoid perpetuation of the inflammatory process and symptoms.
|