Abstract
A case of humerus
fracture associated with malignant fibrous histocytoma in an 83
year old woman is presented. Malignant fibrous histiocytoma of
the bone, is a condition that involves the humerus in 8% of
cases and represents less than 1% of primary bone tumours. The
patient with humeral shaft fracture treated with Hackethals
technique was presented three months later with tumefaction of
the arm and osteolysis in the radiograph. Diagnosis of malignant
fibrous histiocytoma of the bone after humerus fracture was
confirmed by Cancer Antigen 15-3, CA 19-9, gammagraphy, MRI and
biopsy. Early diagnosis with actin antibody HHF35, alpha smooth
muscle actin, bone morphogenic protein-2 (BMP2), human
p52-binding protein (MDM2), p53 gene and p21WAF-1 gene are
emphasized. Treatment options, including surgery, radiotherapy
(15-45 Gy) and chemotherapy (methotrexate, adriamycin,
ifosfamide, cisplatin and doxorubicin, with new alternatives
like ST1571, flavopiridol or Apo2L) are also reviewed.
Key words:
histiocytoma, malignant,
bone, ST1571, Apo2L, humerus, fracture.
J.Orthopaedics 2007;4(1)e4
Introduction:
Malignant fibrous
histiocytoma of the bone (MFHB) is a rare primary disease
representing less than 1% of bone tumours[1]. MFHB occurrs
primarily in long bones (femur 44%, tibia 21% and humerus 8%).
We present a case report of MFHB in humeral fracture of the
elderly, highlighting the importance of early diagnosis, in
preventing later complications. Although imaging techniques or
biopsy could confirm diagnosis, tumour markers are very useful
for the early diagnosis of MFHB when it is suspected in
fractures of the elderly.
Case Report:

A 83-year-old woman had an
accidental fracture of the proximal third of the right humerus,
that was reduced and stabilized by Hackethals intramedullary
bundle pinning. A trephine biopsy of the osteolytic humeral
wound taken at this time provided no pathological findings. The
patient was readmitted three months later after the verification
of a tumoration with stony consistency in the proximal third of
the right arm without either fever or local signs of infection
(Figure 1). No secretions or other data of interest were noted
at the entry zones of the Kirschners wires and shoulder
anteversion and abduction were very painful for the patient.
 Radiography showed that
the Hackethals technique was well tolerated, but with intense
osteolysis at the focus of the fracture (Figure 2). Tumour
markers were requested and normal results for Cancer Antigen
(CA) 15-3 (17.8 IU/ml) and CA 19-9 (5.8 IU/ml) were obtained.
The level of alkaline phosphatase was 161 IU/L (upper normal
limit of 104 IU/L) by biochemical analysis. IgA level was 598
mg/dl Radiography showed that
the Hackethals technique was well tolerated, but with intense
osteolysis at the focus of the fracture (Figure 2). Tumour
markers were requested and normal results for Cancer Antigen
(CA) 15-3 (17.8 IU/ml) and CA 19-9 (5.8 IU/ml) were obtained.
The level of alkaline phosphatase was 161 IU/L (upper normal
limit of 104 IU/L) by biochemical analysis. IgA level was 598
mg/dl
 as compared to the upper normal limit of 390 mg/dL, but
IgG and IgM were within the normal limits. The haemogram was
normal and the ESR was 37 mm/h. Magnetic resonance imaging (MRI)
showed an oval mass (10 x 9 cm), related to the proximal third
of the humerus diaphysis and the deltoid muscle, with lobate
contours of mixed signal and heterogeneous internal structure
(Figure 3). Bone gammagraphy images suggested pseudoarthrosis in
the proximal third of the right humerus (Figure 4). In
addition, a zone of osteolysis was found in the head of the
humerus with a possible haematoma, tumour or abscess in the soft as compared to the upper normal limit of 390 mg/dL, but
IgG and IgM were within the normal limits. The haemogram was
normal and the ESR was 37 mm/h. Magnetic resonance imaging (MRI)
showed an oval mass (10 x 9 cm), related to the proximal third
of the humerus diaphysis and the deltoid muscle, with lobate
contours of mixed signal and heterogeneous internal structure
(Figure 3). Bone gammagraphy images suggested pseudoarthrosis in
the proximal third of the right humerus (Figure 4). In
addition, a zone of osteolysis was found in the head of the
humerus with a possible haematoma, tumour or abscess in the soft
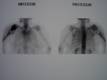 tissue. There was an increase in osteoblastic activity in the
remainder of the bony structures of the upper arm. Senography
of the patient showed mammary fat with calcifications of benign
radiological aspect in both breasts but without radiological
evidence of malignancy and RAPS negative. A biopsy was taken
and pathological examination showed bone material with malignant
fusocellular tumour of storiform pattern which is highly
suggestive of malignant fibro histiocytoma. tissue. There was an increase in osteoblastic activity in the
remainder of the bony structures of the upper arm. Senography
of the patient showed mammary fat with calcifications of benign
radiological aspect in both breasts but without radiological
evidence of malignancy and RAPS negative. A biopsy was taken
and pathological examination showed bone material with malignant
fusocellular tumour of storiform pattern which is highly
suggestive of malignant fibro histiocytoma.
The patient was diagnosed
with malignant fibrous histiocytoma of the proximal third of the
right humerus with pathological fracture (first episode), and
was evaluated by the Oncology Service. After the possibility of
amputation was ruled out, local palliative radiotherapy in
combination with chemotherapy was started, to relieve the
tumefaction of the zone. The patient received analgesia
according to the guidelines of the Pain Unit of our institution.
Discussion :
Malignant fibrous
histiocytoma of the bone (MFHB) manifests as a palpable mass in
half the cases and/or as a painful tumoration in more than 75%
of the cases. MFHB could occur in a spontaneous fracture in 10%
of the cases and is visible in the x-ray as a lytic formation,
metaphysary, often with a moth-eaten appearance of the cortical
reduction. MFHB could appear after radiation, neurofibromatosis
or after osteosynthesis of fractures, as it appeared after the
Hackethals osteosynthesis in the present case report. Schuh et
al.[2] reported a malignant fibrous histiocytoma after hip
arthroplasty.
MFHB diagnosis may be
suspected with gammagraphy, computerized axial tomography or
magnetic resonance imaging (MRI) but it is confirmed only by
histopathology of the biopsy. Different histopathologic forms
such as fibroblastic with fascicular rupture, histiocytic with
vimentin filaments, or similar to giant cell sarcomas may be
observed. Usually, diagnosis of MFHB is made too late as in our
case report. Therefore we suggest that molecular diagnosis is
essential for an early diagnosis of MFHB. Ueda[3] used
anti-muscle actin monoclonal antibody HHF35, alpha smooth muscle
actin (alpha SMA) and bone morphogenetic protein (BMP-2) as
markers for MFHB[4]. Mutations[5] in p53, alterations in MDM2
gene and expression of p21WAF-1 gene have been reported in
histological studies[6].
Pathologies such as benign
giant cell tumours, fibrosarcomas, fibroblastic osteosarcomas
and metastasis of the carcinomas should be considered for the
differential diagnosis of MFHB.
MFHB progresses rapidly as
seen in our case report and can advance quickly via the
lymphatic route, with a survival rate at 15 years of 37% of the
cases. Campanacci[7] reported remission survival rates of 40%
and 21% for patients affected with primary or secondary MFHB,
respectively.
Resective surgery
(including pseudo capsule, better than marginal or contaminated
surgery) and chemotherapy appear to be the most promising
therapeutic alternatives since local control of the illness
could be achieved in 70-80% of cases if the diagnosis and
surgery are performed early[8]. Results depend on the extent of
resection margins, as well as the presence of metastasis,
neoplastic embolisms or metastatic lymphatic nodules.
Our patient received
chemotherapy. Surgery with chemotherapy (methotrexate) is
considered efficacious in 80% of cases with subsequent
functional improvement. The best therapeutic protocol consists
of high pre-operative doses of methotrexate, followed by
extensive resection followed by post-operative chemotherapy with
high doses of methotrexate plus adriamycin, ifosfamide and/or
cisplatin. Using this protocol, remissions are achieved in 60%
of the cases, although others have used doxorubicin and
cisplatin as alternative chemotherapies Recently, imatinib
mesylate STI571 has been considered as a possible
chemotherapeutic agent since it depresses tyrosine-kinase
activity in a study of four malignant fibrous histiocytoma cell
lines (TNMY1, GBS-1, Nara-F and Nara-H) with encouraging
results. Flavopiridol, a powerful inhibitor of the cell cycle
at G1 and G2 phases in vitro, has proven to be effective in
61-64% of the malignant fibrous histiocytoma cell lines[9].
Treatment with cytokines (tumour necrosis factor-related
apoptosis-inducing ligand - TRAIL/Apo2L -) combined with
doxorubicin was described as another new therapeutic alternative
by increasing rate of apoptosis[10].
Finally, our patient
received radiotherapy too, as indicated in cases without
complete surgical eradication of the disease. Radiotherapy
(15-45 Gy) may also be used in combination with surgery for
better local control of the illness in patients without
metastases.
Reference :
-
Joo M, Lee GJ, Koh YC, Kwon OK, Park YK.
Primary intraosseous malignant fibrous histiocytoma of the
skull: a case report. J Korean Med Sci.2003 Aug;18(4):609-13.
-
Schuh A, Zeiler G, Holzwarth U, Aigner T.
Malignant fibrous histiocytoma at the site of a total hip
arthroplasty. Clin Orthop.2004 Aug(425):218-22.
-
Ueda T, Araki N,
Mano M, Myoui A, Joyama S, Ishiguro S, et al.
Frequent expression of smooth muscle markers
in malignant fibrous histiocytoma of bone. J Clin Pathol.2002
Nov;55(11):853-8.
-
Asano N, Yamakazi T, Seto M, Matsumine A,
Yoshikawa H, Uchida A. The expression and prognostic
significance of bone morphogenetic protein-2 in patients with
malignant fibrous histiocytoma. J Bone Joint Surg Br.2004
May;86(4):607-12.
-
Gazziola C, Cordani N, Wasserman B, Carta S,
Colombatti A, Perris R. Malignant fibrous histiocytoma: a
proposed cellular origin and identification of its
characterizing gene transcripts. Int J Oncol.2003
Aug;23(2):343-51.
-
Kawaguchi K, Oda Y, Sakamoto A, Saito T, Tamiya
S, Iwamoto Y, et al. Molecular
analysis of p53, MDM2, and H-ras genes in osteosarcoma and
malignant fibrous histiocytoma of bone in patients older than 40
years. Mod Pathol.2002 Aug;15(8):878-88.
-
Campanacci M, Olmi R. Fibrosarcoma of bone. A
study of 114 cases. Ital J Orthop Traumatol 1977;3:199-206.
-
Buchner M, Bernd L, Zahlten-Hinguranage A,
Sabo D. Primary malignant tumours of bone and soft tissue in the
elderly. Eur J Surg Oncol.2004 Oct;30(8):877-83.
-
Honoki K, Yoshitani K, Tsujiuchi T, Mori T,
Tsutsumi M, Morishita T, et al. Growth
inhibition and induction of apoptosis by flavopiridol in rat
lung adenocarcinoma, osteosarcoma and malignant fibrous
histiocytoma cell lines. Oncol Rep.2004 May;11(5):1025-30.
-
Clayer M, Bouralexis S, Evdokiou A, Hay S,
Atkins GJ, Findlay DM. Enhanced apoptosis of soft tissue sarcoma
cells with chemotherapy: A potential new approach using TRAIL. J
Orthop Surg (Hong Kong).2001 Dec;9(2):19-22.
|

