|
Alok Chhabra*, Amit Goyal, R E Mansel
*Department
of Surgery, Wales College of
Medicine, Cardiff
University, Cardiff, United
Kingdom.
Address for Correspondence
- Alok Chhabra
- Department of Surgery, Wales College of Medicine, Cardiff University
- Cardiff- CF14 4XN, United Kingdom
- Tel: +44 2920744710
- Fax: +44
2920761623
- Email: chhabraa1@cardiff.ac.uk
|
|
Abstract
Soft
tissue sarcoma is a rare tumour and the diagnosis is often not
suspected before biopsy or excision. We report a 72 year old
female with an advanced soft tissue sarcoma who presented
initially with symptoms and signs that mimicked a thigh abscess.
The diagnosis was missed at the time of surgery and only
revealed by the histopathology results of the abscess wall.
Key Words:
abscess, haematoma, malignant fibrous histiocytoma, soft tissue
sarcoma
J.Orthopaedics 2007;4(1)e1
Introduction:
Soft
tissue sarcoma (STS) is a rare tumour of connective tissue
muscle, tendon, blood vessels, nerves and fat (1% of all
malignant tumours). Most sarcomas typically present as a
painless mass and are usually discovered incidentally
following excision of a lump with no prior suspicion that it
could be a sarcoma1. STS can mimic a haematoma or
abscess as haemorrhage and necrosis are not uncommon
features in these tumours. We report a 72 year old female with
an advanced soft tissue sarcoma who presented initially with
symptoms and signs that mimicked a thigh abscess.
Case Report:
A 72 years old
female presented to the GP with four weeks history of pain and
swelling in left hip following trauma from a car door. She had a
past medical history of left hemithyroidectomy for multinodular
goitre and MI. On examination she had a tender swelling 5x3 cm
in size over the left greater trochanter associated with
erythema of overlying skin. Pelvic X-ray showed
minor
degenerative changes in both hips with no other abnormality.
She was
 diagnosed to have left trochanteric bursitis and
treated with antibiotics. Her symptoms deteriorated after some
initial improvement and she was referred to the trauma clinic.
Ultrasound scan of the left hip and upper thigh showed large
loculated irregular fluid collection consistent with a gluteal
abscess. Incision and drainage of the abscess revealed sero-sanguineous
fluid with fibrinous flakes. Fluid sent for culture did not grow
any organisms. Unfortunately, the swelling recurred and a repeat
incision and drainage revealed a large haematoma
intraoperatively. Fluid sent for culture did not grow any
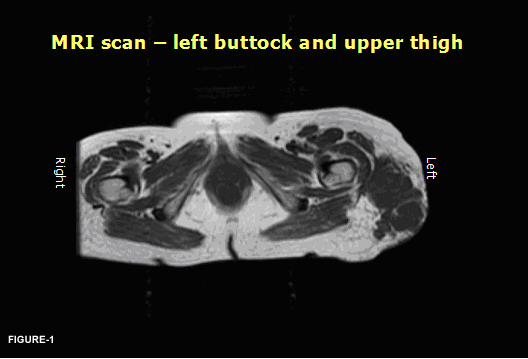
organisms but tissue sent for histopathology showed features
consistent with malignant fibrous histiocytoma. MRI scan revealed large multifocal soft tissue sarcoma in the
left hip and upper thigh (Fig:
1).
Staging CT scan of chest Abdomen, and pelvis did not show any
evidence of distant metastasis. The tumour was treated with
radiotherapy and she had a partial response to the treatment. diagnosed to have left trochanteric bursitis and
treated with antibiotics. Her symptoms deteriorated after some
initial improvement and she was referred to the trauma clinic.
Ultrasound scan of the left hip and upper thigh showed large
loculated irregular fluid collection consistent with a gluteal
abscess. Incision and drainage of the abscess revealed sero-sanguineous
fluid with fibrinous flakes. Fluid sent for culture did not grow
any organisms. Unfortunately, the swelling recurred and a repeat
incision and drainage revealed a large haematoma
intraoperatively. Fluid sent for culture did not grow any
organisms but tissue sent for histopathology showed features
consistent with malignant fibrous histiocytoma. MRI scan revealed large multifocal soft tissue sarcoma in the
left hip and upper thigh (Fig:
1).
Staging CT scan of chest Abdomen, and pelvis did not show any
evidence of distant metastasis. The tumour was treated with
radiotherapy and she had a partial response to the treatment.
Discussion :
Soft
tissue sarcoma is a rare tumour. It commonly affects the limbs
followed by head and neck, trunk and retroperitoneum2.
It usually present as a painless mass but sometime can mimic a
haematoma or abscess. This case highlights that recognition of
these features are important as they may be the initial
presentation of the underlying malignant disease process.
Soft-tissue sarcomas present unique challenges in detection and
treatment. The diagnosis is often not suspected before biopsy or
excision. Surgeons should be suspicious and consider doing a
biopsy in a patient with: 1) the abscess present in the unusual
site like thigh with no specific history, 2) recurrent sterile
abscess and 3) when no pus is found during incision and drainage
of an abscess. Ultrasound is operator dependent and often is
unhelpful in differentiating a soft tissue sarcoma from benign
lesions such as abscess or haematoma. MRI scan or CT scan should
be requested when the diagnosis is in doubt.
Treatment of soft tissue sarcoma is mainly surgical which
includes wide local excision of the tumour. Radiotherapy is
indicated for large and high grade tumours and chemotherapy for
specific tumours like Ewings sarcoma and rhabdomyosarcomas. The
5- year survival rate is 50-60% as a group345.
In
conclusion, tumour size at presentation adversely affects the
patient prognosis. Therefore delay in diagnosis should be
avoided and the patient should be managed by Multi Disciplinary
Team for the best outcome.
Reference :
-
Fletcher CD, et
al., Clinicopathologic re-evaluation of 100 malignant fibrous
histiocytomas: prognostic relevance of subclassification. J
Clin Oncol., 2001. 19(12): 3045-50.
-
Enjoji M, et al.,
Malignant fibrous histiocytoma. A clinicopathologic study of
130 cases. Acta Pathol Jpn., 1980. 30(5):727-41.
-
Ekfors TO and R.
V., An analysis of 38 malignant fibrous histiocytomas in the
extremities. Acta Pathol Microbiol Scand, 1978. 86(1):25-35.
-
Rooser B, et al.,
Malignant fibrous histiocytoma of soft tissue. A
population-based epidemiologic and prognostic study of 137
patients. Cancer, 1991. 67(2): 499-505.
-
Rydholm A, et al.,
Epidemiology of soft-tissue sarcoma in the locomotor system. A
retrospective population-based study of the
inter-relationships between clinical and morphologic
variables. Acta Pathol Microbiol Immunol Scand, 1984. 92(5):363-74.
|

