|
Abstract
Ewings sarcoma sometimes presents with a
pathological fracture in a long bone. We describe what we
believe is the youngest reported case of a nine month old with a
pathological fracture of the right humerus confirmed as Ewings
sarcoma. Multimodal therapy in patients with isolated lesions
offers the best prospect of survival.
Key words: Pathological
fracture, Ewings, infant
J.Orthopaedics 2006;3(1)e6
Case Report:
Ewings sarcoma accounts
for approximately 15% of primary malignant bone tumours with
peak incidence between ages 10 and 20. Recent advances in
surgical management, adjuvant radiotherapy and combination
chemotherapy have significantly improved long term prognosis.
The youngest patients described in the literature to date are
two years old1,2. We report a nine month old infant presenting
with pathological fracture of the right humerus confirmed as
Ewings sarcoma.

A nine month old girl
presented with painful swelling of the right humerus (figure-1).
There was no history of trauma, respiratory symptoms or
constitutional upset. Examination revealed diffuse swelling and
exquisite tenderness along the mid shaft of right humerus
without any distal neurovascular deficit. Plain radiology
showed a pathological fracture through a lytic lesion involving
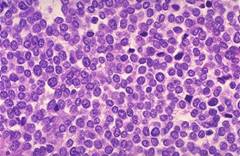
the diaphysis of the humerus. Biopsy of the right humerus
displayed histology consistent with a diagnosis of Ewings
sarcoma (figure 2). Chest and abdominal CT scans did not reveal
any metastases and bone scan showed an isolated lesion in the
right humerus with no other skeletal metastases (figure 3).
However, bone marrow
aspirate suggested
malignant infiltration. There was no clinical or haematological
evidence of bone marrow failure. Various management strategies
and prognosis were discussed with the parents who refused
surgery and radiotherapy, but consented to combination
chemotherapy. Initial response to chemotherapy was satisfactory
and follow up at six months had not shown any relapse.
Discussion :
In children, Ewings
sarcoma is the second most common primary bone tumour, but the
most lethal. It arises from red marrow and is a form of
primitive neuroectodermal tumour. There is a slight male
predominance and it is more common in caucasians.
Clinical presentation is
with intense pain and localized signs of inflammation with
neurological signs in axial skeletal involvement. Pathological
fracture is a rare but recognized presentation. Lungs and bone
marrow are the most common sites for metastases, the presence of
which greatly diminishes prognosis.

Optimal management
involves initial systemic combination chemotherapy followed by
surgery (Reconstructive or ablative) with or without
radiotherapy. Using these strategies in patients with localized
disease, five year survival can be up to 70%1,3,4 . Recognized
factors for a poorer prognosis include male sex, anaemia,
elevated LDH levels, no use of chemotherapy and poor response to
chemotherapy. Good chemotherapy response allows reconstructive
surgery to be performed without a significant increase in
recurrence or metastatic dissemination, whilst poor response may
warrant amputation5 . Inoperable tumours are managed by mega
dose chemotherapy and radiotherapy5,6. In this case unimodal
therapy alone had to be adopted by default.
Conclusion:
Ewings sarcoma should be
considered in the differential diagnosis in an infant with a
pathological fracture of a long bone. Early diagnosis and
multimodal therapy greatly improves outcome.
Reference :
1. Cotterill SJ, Ahrens S, Paulussen M,
Jurgens HF, Voute PA, Gadner H et al Prognostic factors in
Ewing's tumor of bone: analysis of 975 patients from the
European Intergroup Cooperative Ewing's Sarcoma Study Group.
Journal of Clinical Oncology 2000; 18 (17): 3108-14
2. Saenz NC, Hass DJ, Meyers P,Wollner N,
Gollamudi S, Bains M et al. Pediatric chest wall Ewing's
sarcoma. Journal of Pediatric
Surgery. 2000; Apr;35(4):550-5
3. Nesbit ME, Gehan EA, Burgert EO Jr,
Vietti TJ, Cangir A, Tefft M et al. Multimodal therapy for the
management of primary, nonmetastatic Ewing's sarcoma of bone: a
long-term follow-up of the First Intergroup study. Journal of
Clinical Oncology 1990; (10): 1664-74.
4. Sluga M, Windhager R, Pfeiffer M,
Ofner P, Lang S, Dominkus M et al. Osteosarcoma and
Ewing's sarcoma-The most frequent malignant bone tumors in
children-therapy and outcome. Zeitschrift fur Orthopadie und
Ihre Grenzgebiete. 2002; Nov-Dec;140(6):652-5
5. Schovanec J, Mracek J, Havlas V,
Trc T. Ewings sarcoma in children- current surgical
treatment options, evaluation of our patients. Acta Chirigiae
Orthopeadicae Traumatologiae Cechoslovaca .2004; 71(4):220-7
6. Shankar AG, Pinkerton CR, Atra
A. Local therapy and other factors influencing site of relapse
in patients with localised Ewing's sarcoma. United Kingdom
Children's Cancer Study Group (UKCCSG). European Journal of
Cancer 1999; 35 (12): 1698-704.
|

