|
Abstract:
Background: Total hip arthroplasty (THA) for osteoarthritis secondary to developmental dysplasia of the hip (DDH) is technically difficult due to the abnormal anatomy of femur and acetabulum. Surgery may be facilitated by using a modular femoral prosthesis, which allows intra-operative variations in neck length and version.
Objectives: To assess our early results with the S-ROM (DePuy), a cementless modular femoral implant, for hip arthroplasty in patients with DDH.
Methods: 14 hips with DDH (Crowes levels II, III, IV) were operated on between 2007 and 2010 and were evaluated in our clinic. All patients underwent a clinical interview, function and pain evaluation as well as physical examination and radiographic evaluation.
Results: The average follow up time was 18.3 months. Patients reported significant improvement in pain (from 8.4 to 2.2 on the visual analog scale, p<0.001), and significant improvement in hip function (from 29.4 to 66.1 on the Harris Hip Score, p<0.001). None of the arthroplasties have been revised. No radiographic evidence of osteolysis was seen around the femoral or acetabular implants.
Discussion: Our early results with the S-ROM femoral prosthesis for the treatment of DDH were good and correlate with those published involving complex arthroplasty for DDH.
Conclusion
Dramatic decreases in exposure can be achieved by better discipline with the usage of II. This needs to be a fundamental part of registrar training.
The survey shows trainees are not aware, or fail to adhere to current guidelines and that hospitals are not providing appropriate safety equipment and not insisting that staff exercise safe practices.
( ABSTRACT WORD COUNT 250)
J.Orthopaedics 2012;9(4)e3
Keywords:
Arthroplasty, Total Hip Replacement, Developmental Dysplasia of the Hip, Clinical Outcome, Hip Pain, Hip Function
Introduction:
Hip dysplasia is a developmental disorder that results in anatomic abnormalities leading to increased contact pressure in the joint and, eventually, coxarthrosis. The treatment of choice for DDH patients with end stage coxarthrosis is total hip arthroplastyi. However, the hip deformity which these patients present, both in severity and variability, poses a major challenge to the surgeon. Subsequently, hip arthroplasty in patients with DDH has a higher failure rate than for the general population. Total hip arthroplasty using uncemented implants is a relatively new procedure and shows promising results in recent studies .
Difficulty and poorer results in hip arthroplasty is related to the features of the dysplastic hip, among which, deficiency of the acetabulum (anteriorly, laterally and superiorly); anteversion and valgus position of the femur; narrowing of the femoral canal; soft tissue contractures; and shortening of the leg. Hip dysplasia is commonly classified into 4 different levels according to the Crowe classification. This classification is a based on measuring the extent of proximal migration of the femoral head, on anteroposterior radiograph of the hip.
The challenge of hip arthroplasty in DDH, especially Crowe's levels III (75%-100% subluxation) and IV (complete dislocation), brought about modular cementless hip implants, such as Depuy's S-ROM. This implant allows intraoperative variation in femoral neck position (both length and version), and eventually accommodate better to the final acetabular position.
We report our experience using S-ROM cementless arthroplasty for the treatment of Crowe's level II, III and IV over a 4-year period.
methods:
Institutional ethics and a scientific committee approval were obtained for this study.
The study included a series of patients with DDH (Crowe level II, III, IV) who underwent Total Hip Arthroplasty using the S-ROM modular implant (by Depuy) during the years 2007-2011. All surgeries were performed by senior adult reconstructive surgeons of the Tel-Aviv Sourasky Orthopaedic departments.
A total of 11 patients (14 hips) were treated with cementless total hip arthroplasty with the above mentioned implant.
Inclusion criteria for this study were Patients with DDH, Crowe's level II, III, IV; Ability to understand and accept the trial procedures and sign an informed consent form in accordance with national legislation; Patients with non-inflammatory degenerative joint disease, symptomatic despite conservative treatment. Exclusion Criteria were Active or past infection of the hip joint; Revision Surgery ; Comorbidity and general medical condition preventing major surgery.
For the purpose of the study, patients were called for an additional follow up for the most up-to-date physical exam, a review of the most recent imaging as well as for filling out questionnaires regarding past and present clinical condition. Of the 14 patients, 3 were unavailable for clinical follow up.
Data collected for each patient included:
- The medical interview: Basic history and patient's demographics; Review of the surgery report (Including surgical approach, cup size, and stem type); Post operative complications: Hip dislocations, infection, fractures, loosening and revision rate; pain level assessment, using visual analog scale (VAS, 0-no pain, 10-severest pain) for pre-operative hip pain levels and post-operative pain; modified Harris Hip Score for subjective pain and hip function assessment, pre-operatively retrospectively and at follow-up.; and 36 item short form health survey questionnaire (SF-36) for quality of life assessment.
- Physical exam: Ranges of hip motions – adduction, abduction, flexion internal and external rotation; Special exams - limb length discrepancy and Trendelenburg.
- Radiographic assessment based on the most recent hip radiograph: Assessment of endosteal lysis, heterotropic ossification, leg length discrepancy, osteotomy healing and anatomical restoration.
The modification of the Harris Hip Score enables to score hip function without the physical exam components, which we lacked pre-operatively. A correction of summed residual scores was applied to allow for a maximum score of 100. This modification was used previously for hip arthroplasy evaluation.
Statistical analysis we used student t-test to determine differences in normally distributed continuous variables (VAS score and HHS).
Results :
Clinical Results The mean age at the time of surgery was 48 years (range, 25-61 years). The mean duration of follow-up was 18.3 months (range, 1.5-39 months). 5 hips (36%) were classified as Crowe’s level IV, 7 (50%) were level III and 2 (14%) were Crowe’s level II.
The mean Modified Harris Hip Score improved significantly (p=0.0001) from 29.44 points (SD 15.02) preoperatively to 66.11 points (SD 18.04) at the time of the latest follow-up. Pain improved significantly (p=0.0001) from 8.4 points (SD 1.6) preoperatively to 2.2 points (SD 1.8) postoperatively. Patient's quality of life measurement using the SF-36 postoperatively was 55 points (range, 13 to 100 points).
Post operative range of motion averages were: mean 96° flexion (range, 80° to 120°), 42° abduction (range, 25° to 60°), 36° external rotation (range, 15° to 60°) and 15° internal rotation (range, 10° to 30°).
Operative procedure 13 procedures were performed through a anterolateral approach and one procedure was performed using the posterior approach. All procedures were conducted with the patients in the lateral position.
Femoral osteotomy was performed in 6 of the operations; the average amount of shortening was 4.6 cm (range 3 to 6 cm). Femoral strut allografts were used in 5 of the operations, in all of the cases as a result of poor bone quality or intraoperative fracture. 2 acetabular graft augmentations were required and 8 adductor tenotomies were performed. Average acetabular cup size was 45.57 (SD 6) and average femoral stem size was 13.5 (SD 2.3).
Complications Intraoperative fractures occurred in the proximal femoral fragment in three hips and were successfully stabilized by cerclage. No cases of infection, symptomatic deep vein thrombosis, symptomatic pulmonary embolism, were encountered. One patient suffered a partial femoral nerve injury. Two patients complained of metallic taste that persisted since the operation. No cases of dislocations were encountered. Subsequently, no revision surgeries were needed.
Radiographic Results Patients' radiographs showed no signs of osteolysis, heterotopic ossification or other pathologies. Acetabular and femoral Allografts were all incorporated into the native bone (figure 1). Osteotomies also showed good bone healing.
Discussion
DDH is a leading cause of hip arthritis in young adults. Abnormal contact stresses in the dysplastic hip predisposes patients with DDH to develop arthritic changes earlier than seen for patients without dysplasia and revision rates for THA in severely dysplastic hips are significantly higher than revision rates for THA in non-dysplastic hips.
Total hip arthroplasty (THA) is the standard of care when end stage osteoarthritis leads to significant pain and loss of functioni. THA goal in DDH patients is to reconstruct the joint in a way that its function and movement range is as close to normal as possible. The intervention approach is based on the DDH severity and can be assessed using Crowe’s classification by measuring the extent of proximal migration of the femoral head on AP hip radiographiv.
Modular neck prostheses have been shown to be able to recover hip biomechanics and are theoretically useful to overcome the pathological anatomy of DDH patients, .
Off-the-shelf cement-less prosthesis with a modular neck system can correct femoral anteversion, restore femoral offset and compensate for leg-length discrepancy easily and quickly after cup and stem implantation. Cementless stems have shown more long-term survival rates than cemented ones, especially in young patients.
The use of modular implants has become more widespread in the past decade. In addition to the modular head-neck junction, which has been used for years, implants such as the Infinity (Dow Corning Wright, Memphis, Tennessee), the RMHS (Smith-Nephew Richards, Memphis, Tennessee), and the S-ROM (DePuy, a Johnson and Johnson Company, Warsaw, Indiana) give the surgeon the possibility to specifically match the anatomy of the metaphyseal and diaphyseal regions of the femoral canal of an individual patient thus allow intraoperative variation in femoral neck position and better accommodation to the final acetabular position due to narrow femoral implant.
Several reports of successful outcome in short-term and mid-term follow up with the use of the S-ROM prosthesis have been published, , . Our results correlate with these reports. Patients reported significant improvement in pain and hip function. Range of hip motion approached normal values. Our patients’ quality of life measurements were lower than that reported for other THAs. Our average post operative Harris Hip Score was lower than that reported by Glynn et al. and Gul et al. However, the pre-operative score was also lower, thus making the improvement in the hip function similar between studies. Only minor complications occurred and subsequently, no revision surgeries were required. One patient suffered partial femoral nerve injury which manifested as quadriceps atrophy. We couldn't account for this complication since there was no significant lengthening of the femur
Our study has several limitations. Evaluation of common post-operative complications and revision rate is sub-optimal due to the relatively short term follow up time. Recall bias should be considered as part of the evaluation was retrospective.
Conclusions
Our early results with the S-ROM cementless femoral prosthesis for adult patients with severe DDH, Crowe's level II-IV, were satisfactory, and correlate with those from other studies. Additional follow up is imperative to detect common complications. We recommend using this versatile implant for this complex hip deformity
Conflicts of Interests and Disclosures of Funding
No funding was received for this paper. This paper had no pharmaceutical or other industry support.
Figures
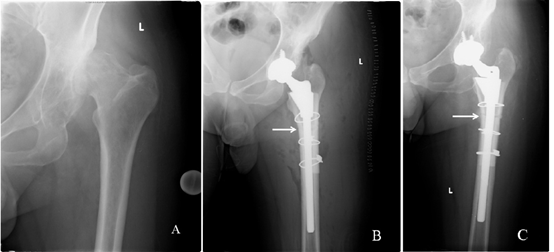
Fig.1 The patient had high dislocation of the left hip (A) and underwent THA with S-ROM prosthesis with subtrochanteric osteotomy (B). Osteotomy bone healing is evident 4 months post operatively (C, white arrows indicate site of osteotomy).
References:
- Sanchez-Sotelo J, Berry DJ, Trousdale RT, Cabanela ME. Surgical Treatment of Developmental Dysplasia of the Hip in Adults: II. Arthroplasty Options. Journal of American Academy of Orthopedic Surgeons 2002;10:334-344
- Sochart DH, Porter ML. The longterm results of Charnley low-friction arthroplasty in young patients who have congenital dislocation, degenerative osteoarthritis, or rheumatoid arthritis. Journal of Bone and Joint Surgery (Am) 1997;79:1599-1617.
- Biant LC, Bruce JMW, Assini JB, Walker PM, Walsh WR. Primary Total Hip Arthroplasty in Severe Developmental Dysplasia of the Hip. Ten-Year Results Using a Cementless Modular Stem. The Journal of Arthroplasty 2009; 24;27-32
- Crowe JF, Mani VJ, Ranawat CS: Total hip replacement in congenital dislocation and dysplasia of the hip. Journal of Bone and Joint Surgery (Am) 1979;61:15-23.
- Noble PC, Kamaric E, Sugano N, Matsubara M, Harada Y, Ohzono K, et al. Three-dimensional shape of the dysplastic femur: implications for THR. Clinical Orthopedic Related Research 2003; 417:27–4
- van den Bekerom MP, Hilverdink EF, Sierevelt IN, Reuling EM, Schnater JM, Bonke H, et al. A comparison of hemiarthroplasty with total hip replacement for displaced intracapsular fracture of the femoral neck: a randomised controlled multicentre trial in patients aged 70 years and over. Journal of Bone and Joint Surgery (Br). 2010;92(10):1422-8.
- Yang S, Cui Q. Total hip arthroplasty in developmental dysplasia of the hip: Review of anatomy, techniques and outcomes. World Journal of Orthopedics. 2012; 3(5): 42–48.
- Brand RA. Hip Osteotomies: A Biomechanical Consideration. Journal of American Academy of Orthopedic Surgeons . 1997;5:282–291.
- Thillemann TM, Pedersen AB, Johnsen SP, Søballe K. Implant survival after primary total hip arthroplasty due to childhood hip disorders: results from the Danish Hip Arthroplasty Registry. Acta Orthopedica. 2008;79:769–776.
- Sakai T, Sugano N, Ohzono K, Nishii T, Haraguchi K, Yoshikawa H. Femoral anteversion, femoral offset, and abductor lever arm after total hip arthroplasty using a modular femoral neck system. Journal of Orthopedic Science. 2002;7(1):62-7.
- Traina F, De Fine M, Biondi F, Tassinari E, Galvani A, Toni A. . The influence of the centre of rotation on implant survival using a modular stem hip prosthesis. International Orthopedics. 2009;33:1513–8.
- Traina F, De Fine M, Tassinari E, Sudanese A, Calderoni PP, Toni A. Modular neck prostheses in DDH patients: 11-year results. Journal Orthopedic Science (2011) 16:14–20
- Perka C, Fischer U, Taylor WR, Matziolis G. Developmental hip dysplasia treated with total hip arthroplasty with a straight stem and a threaded cup. Journal of Bone and Joint Surgery (Am) 2004 86(2):312–319
- Glynn A, Connolly P, McCormack D, O’Byrne J. Use of a cementless modular implant for arthroplasty in developmental dysplasia of the hip: Early results. European Journal of Orthopaedic Surgery & Traumatology; 2005; 15: 105–108
- Gul R, Masterson E. Cementless total hip arthroplasty in the treatment of severe hip dysplasia or dislocated hips. European Journal of Orthopaedic Surgery & Traumatology; 2005; 15: 101–10
- Biant LC, Bruce WJM, Assini JB, Walker PM, Walsh WR. Primary Total Hip Arthroplasty in Severe Developmental Dysplasia of the Hip. Ten-Year Results Using a Cementless Modular Stem. The Journal of Arthroplasty, 2009, 24: 27-32.
- Santić V, Legović D, Sestan B, Jurdana H, Marinović M. Measuring improvement following total hip and knee arthroplasty using the SF-36 Health Survey. Collegium Antropologicum. 2012;36(1):207-12.
- Eggli S, Hankemayer S, Muller ME. Nerve palsy after lengthening in total replacement arthroplasty for developmental dysplasia of the hip. Journal of Bone and Joint Surgery (Br); 1999; 81:843–845
|

