Abstract:
Patients with the bleeding pelvic fracture are clinically unstable. While resuscitative measures are in place, decision needs to be made on definitive control of bleeding. The decision for angiography and embolization to stop arterial bleeding is a difficult one and this study hopes to identify the parameters that may aid in this decision:
Introduction
This study was performed due to the inherent difficulties associated with identifying the parameters necessary to determine if a patient with a traumatic bleeding pelvic fracture would benefit from angiography and subsequent embolization.
Methods
121 patients with traumatic pelvic ring injuries were identified from June 2005 till June 2010, from a single-centre National University Hospital. Out of these 121 patients, 15 patients who underwent angiographic evaluation w ere identified. 11 out of the 15 had angiography and embolization done, while the remaining 4 only had angiography done. Another group of 29 patients who had not undergone angiography were identified from the main population via age-matched criteria and found representative of the main population via 2 samples T test. Systolic blood pressure , base excess, 24 hour fluid and blood requirements, computed tomography findings, Injury Severity Scores(ISS), fracture classifications based on Tiles and Youngs and Burgess classification systems, haemoglobin levels, coagulation profiles were compared between the 15 angiography patients and the 29 non-angiography group of patients.
Results
Angiography group had a larger proportion of patients (80%) with contrast blush noted on contrast-enhanced CT scan(CECT), a higher proportion with unstable pelvic fracture patterns as classified by Tile( B and C fractures) (80%), and Young and Burgess( APC II, III, LCII, III, VS, CM)(92.4%)(p<0.05). Embolized group had higher proportion (81.8%) with hematoma noted on CECT scan, higher proportion with blush on CECT (100%), and higher proportion with unstable fracture patterns (UFPs) (72.7%) as classified by Tile (p<0.05). Positive predictive value for embolization using hematoma alone is 39% while that of blush alone is 73% and unstable Tile fracture alone is 47%. Positive predictive value of combined hematoma, blush and unstable Tile fracture pattern is 75%.
Discussion
Significant factors for angiogram would be unstable pelvic fracture patterns, presence of hematoma and contrast blushing on CT. Further prospective data is required.
J.Orthopaedics 2012;9(2)e2
Keywords:
Introduction
High-energy pelvic fractures are life-threatening injuries. Extensive bleeding associated with these fractures is common. 15% to 30% of patients with high-energy pelvic injuries are hemodynamically unstable which may be directly related to blood loss from the pelvic injury. Hemorrhage remains the leading cause of death in patients with these fractures with an overall mortality rate between 6 to 35%
.
Bleeding associated with pelvic fractures requires efficient evaluation and timely intervention. This almost always necessitates a multidisciplinary approach. Although the general surgery trauma team directs the treatment of the multiply injured person, it is important for the patient with pelvic fracture that the orthopedic surgeon be involved in every phase of treatment including primary resuscitation. Early assessment by an orthopedic surgeon familiar with pelvic fracture patterns allows the treatment team to establish diagnostic and treatment priorities and it expedites the institution of life-saving measures. A thorough understanding of potential sources of bleeding and an awareness of treatment options are essential for all physicians involved.
Patients with pelvic ring disruptions can be generally divided into two groups. The first group comprise of patients who sustain stable pelvic injuries with most of the injury confined to the ligamentous tissues. The second group has patients who sustain displaced pelvic ring fractures either rotationally or vertically unstable and these patients usually require emergency hemorrhage control and a multidisciplinary team approach for management.
One of the most important decisions in a bleeding pelvic fracture is the decision whether to proceed to the interventional suite for pelvic arterial angiogram and embolization. In Singapore hospitals, immediate recognition of instability caused by pelvic trauma is typically followed with resuscitation via ATLS (Advanced Trauma Life Support) principles followed by use of blood products, external mechanical stabilization, followed by decision for intervention. Emergency intervention for the pelvis, besides external fixation can be in the form of angioembolization or extraperitoneal packing. What the literature says about the type of intervention may be controversial but perhaps an understanding of the concepts of the physiology of the bleeding pelvic fracture, with the evidence given in the literature may help to answer some of these questions. Furthermore based on this retrospective study that we have undertaken, certain trends may be observed in the management of bleeding pelvic fractures in our Singapore hospitals.
The bleeding pelvic fracture poses a clinical challenge to even the most experienced of trauma surgeons and none can be managed in a fixed so-called textbook style
.
Ours is a retrospective single-institution study that we undertook at the National University Hospital, Singapore on a patient population of 121 traumatic pelvic fractures over a period of 5 years from June 2005 to June 2010.
The study aims to elucidate and analyze certain clinical parameters on the bleeding pelvic fracture and predictive factors for angioembolization for these fractures. When we examine the bleeding pelvic fracture, the sources of bleeding in a pelvic fracture that should be considered are from the iliac arterial branches, the presacral venous plexus, and a large bulk of fractured cancellous bone. Angiography is an important tool in treating arterial bleeding in hemodynamically unstable patients with pelvic fractures. Indications and proper timing for performing pelvic vessel angiography remains controversial. Part of the purpose of our retrospective study was to evaluate our experience in managing patients with severe pelvic fractures in order to delineate the indicators that might help to identify those patients who may benefit from pelvic angiography and embolization early.
Study Design, Methodology and Results
.
Design and Methods
121 patients with a traumatic pelvic injury sustained from a significant injury i.e. fall from height, road traffic accident were identified from June 2005 till June 2010 from a tertiary trauma centre in Singapore, The National University Hospital. Low energy falls with osteoporotic pelvic fractures were excluded from the study. Some patients in the group identified had concomitant injuries with other surgical issues but were still included in our study based on the pelvic injury sustained.
15 patients who underwent angiography 11 with and 4 without embolization were identified from these 121 patients and the characteristics of this particular patient population were evaluated based on several parameters such as 1. Systolic blood pressure on arrival 2. Base Excess 3. 24-hr fluid and blood requirements 4. CECT findings (contrast enhanced CT) 5. ISS (Injury Severity Scores) 6. Fracture pattern 7. Fracture classification. 8. Hb pre and post angio 9. Coagulation profiles.
Another 29 patients from the main group were age-matched and analyzed. These 29 patients had not undergone angiography. They were also evaluated via 2 sample t-test with the remaining 106(121-15) via parameters stated above and were found representative of the main patient group. Case notes and computer records of patients were traced to identify patients who had undergone angiography and those who had undergone angiography and embolization. The 29 age-matched control cases from the rest of the patients with pelvic fractures were also analyzed and comparisons made with the group that had undergone angiography.
The angiography group and the non-angiography group were age-stratified and analyzed based on the parameters recorded. There were 15 patients in the angiogram group and 29 in the non-angiogram group.
A further sub-analysis was done between the patients who underwent embolization and those that did not have embolization. Amongst the total number (29+ 15) 44 patients analyzed, 11 had undergone embolization and 33 had not.
The results of the study was analyzed using the SPSS program version 17.0.
Results
Among the parameters analyzed between the 2 groups, it was noted that across the age groups, there were a few significant differences.
The mean 1st hemoglobin levels (Hb1) which is the 1st laboratory result that was obtained from the patient on presentation in the Emergency department was significantly lower in the angiography group (mean= 11.13) compared to the non-angio group (mean= 13.12). It was also noted that the angio-group had a lower mean 2nd hemoglobin( Hb2) (mean= 9.28) which is the hemoglobin levels obtained after angiography was performed either with or without embolization.( p<0.05). However it is interesting to note that the mean Hb post angio was lower compared to the Hb pre angio. Although this was not clinically significant when compared to the difference in Hb noted in the non-angio group, the author believes that the reason for this could be continued bleeding from the other sources i.e venous and bone bleeding. Another possibility could be the blood loss that had already occurred in the intervening period before angiogram and embolization was done to stop any bleeding.
( Table 3)
Another conclusion we can draw from the non-significance of the differences in the Hb between the angio and the non-angio group is the effectiveness of angiography.
The angio-group had significantly larger group (12 out of 15)(80%) with blush of contrast noted on contrast enhanced CT scans as compared to the non-angio group (11 out of 29)(10.3%) and this was statistically significant.( p <0.05) (Table 1).
The angio-group had a higher proportion of patients with an unstable pelvic fracture as classified by Tile (80%) (12 out of 15) and Young and Burgess (80%)( 12 out of 15) , and this was statistically significant in this study when compared to the non-angio group of whom the unstable pelvic fracture by Tiles classification was 17.2%( 5 out of 29) and by Youngs and Burgess 48.4%( 14 out of 29).(p<0.05).
Lower mean SBP levels, higher fluid requirements and a higher proportion of associated injuries were noted in angio-group (mean SBP=105mmhg, mean fluids in 24 hrs=2400mls). Nevertheless, these differences were not statistically significant in this study
.
It was noted that whether angiography was done pre or post surgery had no correlation with the stability of fracture as classified by Tile.
The majority of fractures in the angio-population were mostly unstable fracture patterns as shown earlier to be statistically significant. This observation was also noted to be true when Young and Burgess classification fracture patterns were analyzed.
10 out of the 11 fractures that underwent pre-surgery angiography, was noted on CT to have hematoma. Only 50% (2 out of 4) of the patients who underwent angiography after surgery had hematoma on CT.
Further analysis was done between the patients embolized in the angio-group, compared to those that were not. The comparison therefore is between the 11 that required embolization and the 33 that did not require embolization.
Of the 11 embolized 9 showed hematoma on the CECT scan( 81.8 %) as compared to the non embolized group 14/33 ( 42.4%). (p<0.05). Of the 11 embolized, all 11 had blush on CECT as compared to 4 out of the 33 in the non-embolized group. (p<0.05).
72.7% of the fracture patterns in the embolization group were unstable as classified by Tile, compared with the 27.3% in the non-embolized group. (p<0.05).
Positive predictive value for embolization using hematoma alone is 39% (9 out of 23)while that of blush alone is 73%( 11 out of 15) and unstable Tile fracture alone is 47%(8 out of 17). Positive predictive value of combined hematoma, blush and unstable Tile fracture pattern is 75%( 9 out of 12). i.e Out of 12 patients with presence of hematoma, blush and an unstable fracture pattern, 9 of these patients underwent an embolization as they were noted to have an actively bleeding vessel on angiogram.
|
Angio |
No Angio |
P value( chi sq) |
Tile unstable |
12 |
5 |
< 0.05
(0.0005) |
Tile stable |
3 |
24 |
|
|
|
|
Young unstable |
12 |
14 |
< 0.05
(0.007) |
Young stable |
3 |
15 |
|
|
|
|
Hematoma |
12 |
11 |
< 0.05
(0.0008) |
No Hematoma |
3 |
18 |
|
|
|
|
Blush |
12 |
3 |
< 0.05
(0.0005) |
No blush |
3 |
26 |
|
|
|
|
GS injury |
6 |
7 |
> 0.05 |
No GS injury |
9 |
22 |
|
|
|
|
LB fracture |
1 |
7 |
> 0.05 |
No LB fracture |
14 |
22 |
Table 1: Significant categorical variable differences between the angio vs the non- angio group.
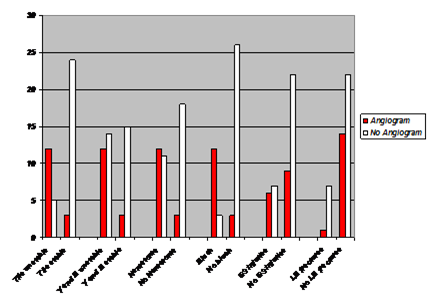
Table 2: Graphical representation of the signifant differences that the angiogram group shares in common.
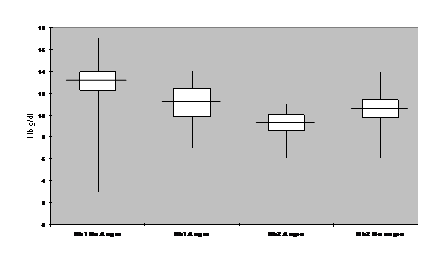
Table 3: Box plot of Hb . Hb1 represents initial Hb on presentation in the Emergency Department and Hb2 is the Hb post procedure. Differences (Hb1-Hb2) is not significant between Angiography and non-angiography group.
Discussion
Angiography and embolization
Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage.
Agolini et al 1 in his 1997 study made a few observations related to the success of embolisation. In his study, he noted that the effectiveness of the angiography was closely tied to the experience of the radiologist, the time it took for angiography to be performed from the time of the injury and ease of transfer of the patient to the angiography suite. A confirmation of successful embolisation was the 1. Reduction in transfusion needs 2. Return of hemodynamic stability 3. Angiography evidence showing no further bleed. This study showed that delayed arrival to the angio suite led to increased mortality.
Velmahos et al 2002 2further confirmed that where facilities exist for angiography, it should be offered early and liberally. The predictors of arterial bleeding that he elucidated from his study was 1) Age more than 55 years old 2) absence of long bone fractures and 3) emergent angiography which further strengthens the case for early angiography. His earlier study in 20003 highlighted the safety and efficacy of angiography and that it can be used as a first-line measure in controlling pelvic bleeding. Furthermore, the advantages of angiography are the possibility that if offered early, bleeding could be controlled by a less aggressive means.
Jen et al 20114
recently confirmed this together with Eastridge et al 2002 5when increased mortality rates were reported when patients with hemorrhagic shock associated with an unstable pelvic fracture and hemoperitoneum underwent laparotomy before angioembolisation for the pelvic fracture. Angiography and subsequent transarterial embolization (TAE) made it possible to treat multiple active bleeders simultaneously and to avoid further trauma of laparotomy in some cases. Control of the arterial hemorrhage before laparotomy also prevents the aggravation of retroperitoneal bleeding due to reduction of the tamponade effect by laparotomy. Some injuries, such as intestinal perforation, are usually not associated with a large amount of bleeding; thus, delaying repairs until the retroperitoneal arterial hemorrhage is controlled by TAE would decrease the overall blood loss. Except in situations such as major mesenteric tear with massive bleeding, contrast extravasation from angioembolization inaccessible vessels, contrast extravasation from intraperitoneal solid organs in patients who remained unstable despite fluid resuscitation, and massive diaphragm rupture with chest compromise, angioembolization was the preferred early mode of therapy.
Huttinen et al 6observed that in 85% of pelvic fracture (23 out of 27 autopsy examinations), bleeding was noted to be from the small arteries at the fracture site. Moreover Bassam et al's 7compelling observations comparing external fixation to primary angiography with embolization for pelvic fractures, noted that despite more severe fractures and greater blood requirements prior to the procedure, the angiography group had fewer complications. No patient who underwent embolization required adjunctive external fixation, while half of the external fixation group required subsequent angiographic embolization. Hence the support for primary angiography and embolization.
While immobilization of fracture fragments will minimize disruption of hemostatic clot, arterial hemorrhage is not likely to be controlled by the external fixator. Operative hemostasis is unlikely to be successful except for the infrequent common or external iliac artery or vein injury. In the hemodynamically unstable patient without evidence of an intraperitoneal or thoracic source, angiography and embolization offer the best opportunity for control of bleeding from deep hypogastric arterial branches or lumbar arteries.
Verbeek et al 8and Heetveld et al 9emphasized on the management of traumatic bleeding pelvic fractures according to guidelines and a decision-making tree. They noted that hemorrhage related mortality was high in the group that underwent laparotomy and the high negative laparotomy rates were to a significant extent due to lack of guidelines governing management. They found that timely angioembolization and orthopaedic intervention is important for hemorrhage control. Persistent bleeding requires decision making within 90 minutes as to whether patient should proceed to laparotomy and pelvic packing or angioembolization. Heetveld et al also recommended early non-invasive
stabilization of the pelvis (C-clamp and binder) followed by angiography within 90 minutes if no intraabdominal bleeding is discovered.
Jeroukhimov et al 10observed that high pelvic AIS, low base excess and increased transfusion requirements were predictive for early angiography. These were indicators of arterial bleeding and in this group of patients; recommendations for liberal and early angiography were made. Angiography should be done early in these patients to allow for time for other interventions if required. Nevertheless, no parameter is good enough on its own to determine arterial bleeding and need for angio. A high amount of clinical decision making is required when it comes to the bleeding pelvic fracture.
The C-clamp and adjunctive embolization appears to be as efficient in controlling hemorrhage as the C-clamp associated with laparotomy and pelvic packing as observed by Sadri et al. 11In those hospitals where angiography facilities are available, it seems reasonable to recommend that patients who remain hemodynamically unstable after rapid application of the C-clamp be treated with arterial embolization as opposed to performing a laparotomy and pelvic packing with its increased risk of mortality and morbidity. Although the C-clamp was effective in controlling hemorrhage in the majority of patients in this review, 36% required arterial embolization to control hemorrhage.
Intravascular compartment fluid replacement is the single most important and effective therapy in the bleeding pelvic fracture with the majority of patients requiring nothing further. 12 But more than just the absolute quantity of fluids that are given, what is noteworthy is the concept of ' controlled resuscitation'. Fangio et al reported the use of vasopressors in the bleeding pelvic fracture to achieve certain blood pressure goals.
Increased arterial pressure may worsen patients outcome by causing rebleeding via disruption of clots and fluid overload causing acute lung injury. 13 Experimental data support the concept of controlled resuscitation in restoring intravascular volume while respecting homeostatic mechanisms.
14 Fangio's paper extrapolated the experience of hypotensive resuscitation from penetrating injuries to blunt injuries and observed similar positive results.
In Fangio's paper, angiography is proposed as a main part of the protocol for management if transfusion requirements exceed 4 units in 24 hrs and there is no extrapelvic/intraperitoneal bleeding. Nevertheless, he still maintains that the question of angiography is controversial. Miller et al 15 claims active pelvic bleeding in 73% of hypotensive non-responders, suggesting that the proportion of arterial injuries is quite high and this is also noted in Huttinen's autopsy studies which shares the same observation.
The opponents to early angiography mainly cite the time element as the major downside to early angiography. It is thought to be time consuming and some studies have claimed 10 hours between admission and angio. 16 Moreover, the availability of an in-house radiologist and the ability to resuscitate patients in the angiography suite if they deteoriate are some of the concerns cited. Some of these concerns and fears lead trauma teams to discount primary angiography as a feasible and perhaps even the most important step in the management of the bleeding pelvic fracture.
The arguments against implementation of the arteriographic treatment limb are often logistic and to some extent surmountable. 17
When angio is used as the main modality of treatment, patient selection is most important, together with the knowledge that angio may need exploration of intraabdominal vessels and hepatic and splenic bleeding can be treated with selective embolization. 18
Based on our study, an analysis of the angiogram cohort, revealed that 11/15 had angio before surgery as compared to the 4 after surgery. Out of the 4 who had angio after surgery, 3 were FAST positive and needed stabilization in OT first with a laparotomy, packing and external fixation due to hemodynamic instability not corrected with fluids and blood transfusion. Angio was subsequent to that due to continuing hemodynamic instability. This was despite packing and external fixation in these 3 patients. One eventually died. As revealed by Verbeek and Heetveld, our studys observation seemed to echo the higher mortality rate in the post laparotomy angio group as opposed to the pre-surgical angio group.
Of the 11 who had angio before surgery, only 2 were FAST positive. Out of these 11, 8 were embolized and 3 were not. There was 1 mortality out of the 8 embolized from cerebral injuries and a traumatic aortic arch injury. Our study revealed also the significantly lower Hb levels noted in the angio vs non angio groups. (p<0.05)
Lower mean SBP levels, higher fluid requirements and a higher proportion of associated injuries were noted in angio group (mean SBP=105mmhg, mean fluids in 24 hrs=2400mls) as compared to the non-angio group.
Pelvic fracture patterns
Pelvic fracture patterns based on classifications and certain observable parameters could be used as a predictor of severity of injury, prognosis and arterial bleeding, which leads us to better manage the patient.
Cryer et al found that 50±70% of patients with disruption of the pubic symphysis or fractures of the pelvic ring with 5 mm or greater distraction will require more than four units of blood, and 30±49%will require more than ten units.
In Tachibana et al, both instability of the pelvic ring and injury severity were correlated with mortality of patients with pelvic ring fractures. Thus, all parameters adopted in the study; Tiles classification, ISS (Injury Severity Score), RTS (Revised Trauma Score), Ps (Probability of survival) could be regarded as potent predictive factors for death of the patients. Assessment of the patient condition in various aspects is thought to be critical in
the initial clinical evaluation. Tiles classification significantly correlates with mortality, and thus is a useful classification system for management of patients with pelvic fractures. Moreover, a close relationship between fracture stability as assessed by this system and injury severity was also suggested. In the treatment of patients with pelvic fractures, surgeons should evaluate fracture stability and injury severity immediately after admission to predict the prognosis and establish the initial treatment plan.
Velmahos et al suggested there are 3 types of ring fractures thats are associated with arterial bleeding.
1. Open book
2. Posterior fractures
3. Pubic rami fracture
in his study which was considered potentially dangerous.
Miller et al noted that fracture patterns of APCII, III, LCII, III, VS and CM are more likely to have arterial bleeding, as well as fractures through the sciatic notch ( due to proximity of the superior gluteal artery).
This was further confirmed by Eastridge at al whenSFPs (LC I, APC I) and UFPs (APC II, III, LC II, III, VS and CM) were compared. SFPs being stable fracture patterns and UFPs being unstable fracture patterns.
Study suggests that once patient is in shock and is undergoing resuscitation, pelvic fracture patterns determine the next step in management or rather are useful in determining treatment. In SFPs, intraperitoneal bleeding seems to be the most substantial factor giving rise to shock, which would probably require laparotomy and its important to have this at the back of the mind even in the case of negative FAST study. In UFPs, shock was mostly from the pelvic source, and if still persistent despite binder techniques and resuscitation, angio is probably the best way forward. If patient presents with an UFP together with intraperitoneal bleeding and is in shock, the options would be laparotomy with pelvic ex-fix at the same time KIV angioembolisation or angioembolisation first then ex fix KIV laparotomy. In this study the UFP and intraperitoneal injury that underwent angio had a 25% mortality rate compared with the group that underwent laparotomy 1st who had a 60% mortality rate.
Our study did show significance in correlation of Tiles and Young and Burgess Classification of stability of fracture patterns when comparing the angio and non-angio groups.
The angio group had a higher proportion of patients with an unstable pelvic fracture as classified by Tile (80%)and Young and Burgess(80%), and this was statistically significant in this study when compared to the non-angio group of whom the unstable pelvic fracture by Tiles classification was 17.2% and by Youngs and Burgess 48.4%.(p<0.05).
Furthermore, when comparing embolization vs non embolization 72.7% of the fracture patterns in the embolization group were unstable as classified by Tile, compared with the 27.3% in the non-embolized group. (p<0.05).dults
Summary and conclusion
Our study aimed to identify the predictive parameters for pelvic angiography in a view to ensuring early embolization is done for the patient with the bleeding pelvic fracture who needs it most.
It is noteworthy that CT with contrast blush, presence of hematoma and an unstable pelvic fracture pattern as defined by Tile would herald a need for angiography emergently as elucidated in our study.
However we must note at the end of the day that managing the pelvic fracture, especially a bleeding pelvic fracture involves more than just the arteries. The other sources of bleeding should be arrested as well with the aid of external fixators and if need be pelvic packing.
The author hopes that a prospective study can be carried out to support the findings of this paper.
References.
Agolini et al Arterial Embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage. The Journal of Trauma: Injury Infection and Critical care Sept 1997 395-399
Velmahos et al A prospective study on the safety and efficacy of angiographic embolization for pelvic and visceral injuries. J Trauma; 2002; 52: 303-308
Velmahos et al Angiographic embolization for intraperitoneal and retroperitoneal injuries. World J Surgery 2000 539-545
Jen et al Angioembolization and laparotomy for patients with concomitant pelvic arterial hemorrhage and blunt abdominal trauma. Langenbecks Arch Surg 2011 396:243250
Eastridge et al The importance of fracture pattern in guiding therapeutic decision-making in patients with hemorrhagic shock and pelvic ring disruptions. J Trauma 2002 53:446451
Huittinen V et al Postmortem angiography and dissection of the hypogastric artery in pelvic fractures. Surgery 1973: 454±462
Bassam D et al Protocol for the initial management of unstable pelvic fractures. Am Surg 1998 64: 862±867
Verbeek et al Acute Management of Hemodynamically Unstable Pelvic Trauma Patients: Time for a Change? Multicenter Review of Recent Practice. World J Surg 2008 32:18741882
Heetveld et al Hemodynamically Unstable Pelvic Fractures: Recent Care and New Guidelines World J. Surg 2004; 28, 904909
Jeroukhimov et al Selection of patients with severe pelvic fracture for early angiography remains controversial. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2009.
Sadri et al Control of severe hemorrhage using C-clamp and arterial embolization in hemodynamically unstable patients with pelvic ring disruption Arch Orthop Trauma Surg 2005 125: 443447
O'Neill et al Angiographic findings in pelvic fractures. Clin Orthop Rel Res 1996; 329: 60±67
Eberhad et al. Initial severity of metabolic acidosis predicts development of acute lung injury in severely traumatized patients. Critical Care Medicine 2000 28; 125-131
Capone et al. Improved outcome with fluid restriction in treatment of uncontrolled hemorrhagic shock. J Am College of surgery. 1995
Miller et al. External fixation or arterigram in bleeding pelvic fracture: initial therapy guided by markers of arterial hemorrhage. J Trauma 2003; 54:437-443
Gansslen et al. Hemorrhage in pelvic fracture. Who needs angiography? Curr opinion Crit care. 2003 ; 9: 515-523
Gylling SF et al. Immediate external fixation of unstable pelvic fractures. Am J Surg 1985
Menachem et al. Hemorrhage associated with pelvic fractures: causes, diagnoses, and emergent management AJR Am J Roentgenol 1991
|

