Abstract:
Background
. Replantation after ectopic temporary implantation of extremities is a new method proposed mainly for the salvage of amputa amputated ted extremities under complex and difficult clinical conditions. Internationally, systemic injuries such as complex amputation of extremities complicated with hemorrhagic shock and multiple organ injuries make a long replantation procedure untolerable for patients, therefore become the contraindication for replantation of amputated extremities, and most patients will be disabled due to amputation of extremities. But if amputated extremities complicated with systemic critical injuries are implanted immediately to ectopic recipient site for temporary survival in the simplest way according to the technical principles of replantation after temporary ectopic implantation of amputated extremities and then replanted to their anatomic sites after general condition and injuries have been improved, this forbidden area for microsurgical replantation of amputated extremities might be broken through that will sustain extremities intact and reduce the rate of disability to the maximum extent.
Methods.
The group included two patients, both male and aged at 31 and 16 years respectively. One suffered crush and avulsion injury at the level of ankle complicated by systemic multiple fractures, hemorrhagic shock, and the other suffered burn and avulsion injury by stangulation at the level of ankle joint with circumferential soft tissue burns and hemorrhagic shock. The times after ectopic implantation of amputated foot were 156 and 108 days respectively. After replanted foot survived, PT and OT rehabilitation trainings were carried out immediately and combined with 10-11 years ( 10.5 years in average) follow-up.
Results
. Their protective superficial sense of skin below ankle joint of replanted foot was restored. The patients could return to carry out light manual work, have no difficulty in daily life and walk freely. In accordance with Chen's standards[10] for evaluation of functional restoration of lower extremities replanted, the restoration of function was evaluated as II grade. The patients were satisfactory with functional recovery of their own foots.
Conclusion.
Replantation after temporary ectopic implantation of amputated extremities is a new method proposed mainly for the salvage of amputated extremities under complex and difficult clinical conditions.
J.Orthopaedics 2011;9(1)e2
Keywords:
Ectopic temporary implantation; Replantation; Amputated extremities.
Replantation after temporary ectopic implantation of amputated extremities is a new method proposed mainly for the salvage of amputated extremities under complex and difficult clinical conditions. Internationally, systemic injuries such as complex amputation of extremities complicated with hemorrhagic shock and multiple organ injuries make a long replantation procedure untolerable for patients, therefore become the contraindication for replantation of amputated extremities, and most patients will be disabled due to amputation of extremities. But if amputated extremities complicated with systemic critical injuries are implanted immediately to ectopic recipient site for temporary survival in the simplest way according to the technical principles of replantation after temporary ectopic implantation of amputated extremities and then replanted to their anatomic sites after general condition and injuries have been improved, this forbidden area for microsurgical replantation of amputated extremities might be broken through that will sustain extremities intact and reduce the rate of disability to the maximum extent.
Since Godina.M[1] first reported a case of successful replantation after temporary ectopic implantation of an amputated hand, a number of reports on the salvage of amputated body parts and organs including finger, limb, penis and scalp with this technique have been documented in the world[1-7]. We totally finished two cases of the replantation of temporary ectopic implantation of an amputated foot for the salvage of lower extremities (from November 2000 to September 2001)[8-9]. After 10-11 years ( 10.5 years in average) follow-up, some results were accomplished and summarized as follows:
1. General Information
The group included two patients, both male and aged at 31 and 16 years respectively. One suffered crush and avulsion injury at the level of ankle complicated by systemic multiple fractures, hemorrhagic shock, and the other suffered burn and avulsion injury by stangulation at the level of ankle joint with circumferential soft tissue burns and hemorrhagic shock. The times after ectopic implantation of amputated foot were 156 and 108 days respectively. After replanted foot survived, PT and OT rehabilitation trainings were carried out immediately and combined with 10-11 years ( 10.5 years in average) follow-up. The effects of replantation of lower extremities were evaluated in accordance with Chen's standards: Grade I Return to previous work,normal gait walk,almost normal ROM of knee and ankle joints; Grade II Light work,walk with slight limp,good sensory recovery,ROM =40% of normal; Grade III Useful in daily life,use of higher heel,sensibility reduction but no trophic ulcers; Grade IV Use of crutches,no sole sensation,trophic ulcers. The recipient sites were also followed up that showed the sensory and motor functions were normal, and blood supply and circulation of extremities were also good (Table 1 and Table 2). In both two patients, latissmus dorsi myocutaneous flap was transferred to repair the soft-tissue defect. The follow-up proved that latissmus dorsi could make stretch, adduction and external rotation of humerus, and pull up the limbs when climbing, showing its functions were normal.
Table 1 General Information of Patients
No. Gender Age (years) Diagnosis |
1 Male 31 I Comminuted fracture of intertuberosity of left femur,
severe crush and laceration injuries of left lower
extremity
II Left foot was completely amputated at the level of the
ankle
III Hemorrhagic shock
2 Male 16 I Left foot was completely amputated at the level of the
ankle joint.
II Circumferential devastating burn injury in soft tissue at
the level of left ankle.
III Hemorrhagic shock. |
table 2 Results
No. Time after implantation Function of Recipient site andwhether
( days) replanted extremities the dysfunction occurred |
1 156 II Lower part of right extremity No
2 108 II Lower part of right extremity No |
2.1 Case 1
Patient Mr. Hao, male, 31 years old, suffered a crush injury to his left foot by machinery, resulting in the amputation of left foot. When he arrived at our hospital, A comminuted fracture of intertuberosity of left femur was detected, and a large circumferential laceration wound was found proximal to the amputation stump. Left foot was completely amputated at the level of the ankle ( Figure 1a ) complicated with hemorrhagic shock.

Figure 1a Left foot was completely amputated at the level of the ankle
2.1.1 Replantation after temporary ectopic implantation of amputated extremity was performed on the patient.
The time of warm ischemia for amputated foot arrived at 6 hours, and the patient was complicated with hemorrhagic shock, therefore no condition for primary replantation existed, but the family and patient strongly desired the replantation of foot. We decided finally to undertake replantation after temporary ectopic implantation of amputated foot ( Figure 1b, 1c, 1d ).
 
Figure 1b Amputated left foot was ectopically implanted onto right ankle.
Figure 1c X-ray imaging after surgery: The blood circulation of left foot implanted was reestablished.

Figure 1d Ectopically implanted left foot survived at recipient site, and proximal stump defect of amputation was repaired by latissmus dorsi myocutaneous flap.
2.1.2 After replanted left foot survived after surgery, it was treated with functional rehabilitation.
Immediately after replanted foot survived, PT treatment was applied (10 days or so after surgery), including: concentric massage, mild passive motion of proximal and distal potion of toes of replanted foot and unfixed joint in normal foot to avoid to affect normal joint activity due to long term immobility, knee and hip flexion exercise in bed 3 weeks after surgery with activity levels and scope from little to large, from weak to strong, functional training of toes and ankle joints under non-weight-bearing status, the avoidance of premature walking bearing weight to cause bone nonunion of foot because the aim of foot replantation is to recover its walking and weight-bearing function. Hyperbaric oxygen therapy began 2 weeks after surgery, with oxygen pressure at 0.2 MPa, 60 minutes each time, once daily, totally 10 times. Three weeks after surgery, bone union of foot was confirmed through X-ray reexamination for weight-bearing walking. Eight weeks after surgery OT treatment was applied with protective sense training: when sensory function of replanted foot was completely lost, the patient was instructed to master the approach of visual compensation and avoid the exposure to excessively hot, cold and sharp and heavy objects; positional sense training: after the recovery of protective sense of foot, the therapist stimulated replanted foot with a pencil rubber repeatedly, and instucted the patient to sense the feeling of stimulation points in eye-closing and straightly-looking statuses; dynamic and static touch sense training: the therapist slided and pressed on replanted foot with a pencil rubber with the intensity varying from heavy to light and repeated stimulation of toes of replanted foot, and instructed the patient to sense and identify related feeling repeatedly through eye-closing, eye-opening and eye-closing training to make the patient gradually able to distinguish between the two different touch sense, and the therapist also stimulated the toes with 30 Hz and 256 Hz tuning forks repeatedly to promote the recovery of sense of 256 Hz vibration; discriminative sense training: when the sense of 256 Hz vibration of patient was recovered, and discriminative sense of two points began to appear, the late stage of training was started, some daily necessities like small ball and screws were selected to be placed in clothing pouch, box or pot, the patient was instructed to touch and move these objects with toes and identify them, through eye-closing, eye-opening and eye-closing training, the patient finally could distinguish different objects when the eyes were closed; desensitization training of sensory nerve: firstly, replanted foot was wrapped with dry towel and treated by means of massage, then desensitization therapy was performed by stepping on millet, rice, mung beans, soybeans, metal objects with replanted foot.
2.1.3 Results
Through 10.5 years of follow-up, protective superficial sense of skin below ankle joint of replanted foot was restored. The patient could return to carry out light manual work, have no difficulty in daily life and walk freely. In accordance with Chen's standards[10] for evaluation of functional restoration of lower extremities replanted, the restoration of function was evaluated as II grade. The patient was satisfactory with functional recovery of his own foot ( Figure 1g, 1h, 1i ).

Figure 1g 10.5 years after surgery, the sensation, motion and blood circulation of recipient site of right leg were normal, left foot survived, and the ankle joint was fixed at the position of 90 degree.
 
Figure 1h 10.5 years after surgery, the patient could stand on one leg affected and squat down.
 
Figure 1i 10.5 years after surgery, X-ray imaging film of anteroposterior view of right hip and anteroposterior and lateral view of ankle joint: The complete union of comminuted fracture of intertuberosity of femur and bone fusion of ankle joint were observed.
2.2 Case 2
Patient Mr. Hao, male, 16 years old, presented in our hospital with his left foot completely severed by a hot steel slice. His left foot was completely amputated from the level of the ankle joint combined with extensive burn injury in soft tissue and hemorrhagic shock ( Figure 2a ).
2.2.1 Replantation after temporary ectopic implantation of amputated extremity was performed on the patient.
Since the time of warm ischemia for amputated foot arrived at 3 hours combined with skin defect in left ankle, necrotic zone of circumferential burn injury was difficult to evaluate, the transplantation of latissmus dorsi couldn't be performed at primary stage. But our hospital has the experience of temporary ectopic implantation of amputated foot, therefore it was finally decided that temporary ectopic implantation of amputated foot and foot replantation at the second stage were performed ( Figure 2b ).
 
Figure 2a Left foot was amputated at the level of ankle joint, and burn injury was found in proximal stump, and the boundary of necrotic zone was unclear.
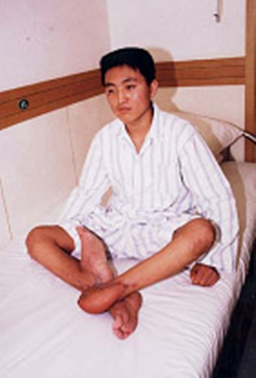
Figure 2b Left foot was implanted ectopically onto right leg, and survived
2.2.2 After replanted left foot survived after surgery, it was treated with functional rehabilitation (the same with those treatments in Case I ).
2.2.3 Results
Through 11 years of follow-up, protective superficial sense of skin below ankle joint of replanted foot was restored. The patient could return to carry out manual work, have no difficulty in daily life, walk and run freely. In accordance with Chen's standards[10] for evaluation of functional restoration of lower extremities replanted, the restoration of function was evaluated as II grade. The patient was very satisfactory with functional recovery of his own foot ( Figure 2c, 2d )
 
Figure 2c 11 years after surgery, the patient could stand on one leg affected and squat down. The sensation, motion and blood circulation of recipient site of right leg were normal.

Figure 2d 11 years after surgery, X-ray imaging film of anteroposterior and lateral view of ankle joint: the bone fusion of ankle joint were observed well.
Discussions
3.1 Preservation methods of amputated extremities
The fundamental purpose of replantation of amputated extremities is to reconstruct the blood circulation of amputated extremities and finally achieve good restoration of their functions. Therefore how to preserve amputated extremities to minimize tissue damage caused by ischemia and extend the activity of tissue cell became the crucial factor to improve success rate of replantation of amputated limb. Current preservation methods of amputated extremities include cryopreservation[11, 12, 13], cryopreservation with organ-preservation solution[14, 15], cryopreservation with perfusion solution[16, 17, 18], hyperbaric oxygen preservation[19, 20, 21], and temporary ectopic implantation[8, 9] that is a kind of completely novel method for the preservation of amputated extremities with the longest storage time, the best effect and the most confirmed success rate by far.
3.2 The indication of replantation after ectopic implantation
Some researchers[21] suggested that surgeon should consider to apply the replantation after ectopic implantation under the following conditions: The anatomic replantation at primary stage was predicted to cause extensive soft tissue necrosis, infection, scarred healing and influence normal functions; it was expected to avoid segmental soft-tissue loss brought by radical debridement; the effective length of amputated extremity was desired to be preseved. Meanwhile, before the replantation after ectopic implantation was decided, all alternative treatment should be excluded such as soft-tissue transplantation to eliminate the wound and abandon the amputated extremity, the replantation of amputated extremity at primary stage after appropriate shortening, soft tissue transplantation while the replantation of amputated extremity was performed in order to preserve the effective length of limb. We thought, besides the above indications under local conditions, when the patient in critical conditions like combined life-threatening complex injuries and traumatic shock cannot tolerate a long procedure of replantation, the replantation after temporary ectopic implantation should be chosen. This is absolutely indicated for the replantation after ectopic implantation, and the others are relative indications.
In Case 1, the patient suffered complex injuries, the time requirement for primary replantation of amputated extremity far exceeded its time limit, therefore only the amputation of extremity could be performed finally if the replantation after ectopic implantation was undertaken.
In Case 2, the patient suffered burn injuries by strangulation, the boundary of local tissue necrosis was unclear, only the replantation after ectopic implantation could be chosen to preserve the effective length of lower extremity and reduce the risks of replantation at primary stage. We anastomosed posterior tibia artery totally for four times in the implantation so as to restore the blood supply of artery which was considered to be caused by extensive intimal damage of long segment of blood vessel in amputated foot by strangulation and inadequate removal of blood vessel. The above situation demonstrated that with the existence of extensive tissue defect in amputated extremity, free tissue transplantation must be carried out firstly to repair tissue defects of left leg and blood vessel[8, 9]. In particular, we emphasized that if the distal stump of extremity injured was preserved relatively well, and had functions after replantation, but the soft tissue of the proximal stump of extremity was severely damaged and had no nerves, blood vessels and tissue connection for anastomosis, the replantation after ectopic implantation could be considered to be performed.
3.3 The selection of recipient site for temporary ectopic implantation and the influences on its function
The selection of recipient site for temporary ectopic implantation is crucial for the success of surgery. The recipient site should have the following conditions: The anatomy of recipient vessels is consistent, and these vessels are easy to approach and dissect; at the second stage of replantation, the recipient can provide a long vascular pedicle to the harvested amputated parts to avoid vascular grafting, the harvest of amputated parts will not compromise the function of the recipient site; the recipient site is in favor of the fixation of amputated extremity, the implantation has little influences on daily life of the patient; the patients' desires and the feasibility of surgery should be considered[8, 9]. We thought contralateral healthy extremity as the recipient site for amputated extremities has many unique advantages. Besides the large diameter and superficial position of blood vessels in this site for easy microvascular anatomosis and dissection of these vessels, a cross-arm or a cross leg flap can be designed in replantation at secondary stage to ensure the survival of amputated extremities. Meanwhile, the second blood-supply system could be established and after it was confirmed by a postoperative angiography, the tube flap could be divided. In both two cases of the group, contralateral implantations were carried out.
Whether temporary ectopic implantation of amputated extremity will cause the dysfunction of recipient site is an issue that we must consider in the surgery. Through 10.5 years of the follow-up study on the recipient site on contralateral extremities in the group, it was found that their sensation, motion and blood circulation were normal.
3.4 The uses of latissmus dorsi myocutaneous flap in replantation after temporary ectopic implantation
In the group, latissmus dorsi myocutaneous flap was used to repair soft tissue defect and bone exposure of the distal stump mainly because the diameter of its blood vessel are large, its anatomy is consistent, and the blood in the flap is well circulated. Only the internal part of latissmus dorsi was separated as myocutaneous flap that didn't affect its normal function. The skin at the donor site of myocutaneous flap and subcutaneous tissue were sutured directly without skin grafting, leaving only a linear scar. Latissmus dorsi of donor site of patients in the group can make extension, adduction, internal rotation of humerus, and pull up extremities when climbing, has normal functions. So we believed that latissmus dorsi myocutaneous flap played a good role in replantation after temporary ectopic implantation and reconstruction of functions.
3.5 The factors that influenced the therapeutic effects of replantation after temporary ectopic implantation
When the surgical physicians decided to perform replantation after temporary ectopic implantation, they must recognize the functions of late second-stage replantated extremity will not be fully regained when compared to primary replantation. Poor postoperative function recovery was reported in previous replantation of temporary ectopically implanted extremities. The replanted extremities(fingers) only have the fixing function during working with little mobility. However, considering the effect of psychological pressure caused by amputation on the patient, the application of temporary ectopic implantation of amputated parts for the salvage of extremities is still clinically valuable. When compared to arm or finger replantation, the demand for function recovery in replantation of lower extremity or foot is relatively lower, restoration of sensation and weight-bearing function usually satisfied the patients. Therefore, the method of temporary ectopic implantation of amputated parts and second-stage replantation is an ideal treatment for amputation of a foot or lower extremity with the specific conditions.
In both two cases, there were good effects observed on the patients with amputation of lower extremity, and no difficulty in daily life. One patient returned to carry out light manual work, and the other patient resumed to perform previous work,and can walk, run and has sports.
In two cases, amputated extremities were replanted to their anatomic sites 156 and 108 days after temporary ectopic implantation respectively. Denervated skeletal muscle atrophy has occurred that caused the decrease and loss of motor function, Therefore we proposed that amputated extremities should be replanted to anatomic site as soon as possible to repair sensory-motor nerve in order to ensure the effect of replantation.
Integrated Treatment Concept[22, 23] has very large influences on functional recovery of replanted extremities that includes primary replantation surgery, the following transfer of tendon and muscle, the union of joint, the orthopedic of joint capsule, bracing application and so on. The participation of physical therapists, occupational trainers, psychological therapists and social workers, etc are needed to achieve better effects in the treatment. Functional reconstruction at late stage played an important role in the recovery of limb function. .
References.
[1] Ono H, Nakagawa Y,Mizumoto S, et al. Evaluation of vascular compliance and vasoconstractive reaction in amputated hind-limbs of rats. J Orthop Res,1995;13(3):375
[2] Ono H, Nakagawa Y, Mizumoto S, et al. Vascular compliance and vasconstractive reactions in rat hind limbs comparison between storage temperature of -1? and 4?. J Reconstr Microsurg, 1997;13(6):409
[3] Bolognesi MP,Chen LF,Seaber AV,et al.Protective effect of hypothermia on contractile force in skeletal muscle. J Orthop Res,1996;14(3):390
[4] St Peter SD , Imber CJ , Friend PJ . Liver and kidney preservation by perfusion [J ] . Lancet ,2002 ,359 (9306) :604-613.
[5] Mowlavi A , Neumeister MW, Wilhelmi BJ , et al. Local hypothermia during early reperfusion protects skeletal muscle from ischemia-reper fusion injury[J ] . Plast Reconstr Surg ,2003 ,111 (1) :242~250.
[6] Wilson YT , Lepore DA , Riccio M , et al. Mild hypothermia protects against ischemia-reperfusion injury in rabbit skeletal muscle[J ] . Br J Plast Surg , 1997 ,50 (5) :343~348
.
[7] Sanger JR, Logiudice JA, Rowe D,et al. Ectopic scalp replantation: a case report. J Plast Reconstr Aesthet Surg. 2010 Jan;63(1):e23-7. Epub 2009 Jun 16.
[8] Wang JN, Tong ZH, Zhang TH,et al. Salvage of amputated upper extremities with temporary ectopic implantation followed by replantation at a second stage. J Reconstr Microsurg. 2006 Jan;22(1):15-20.
[9] Wang JN, Wang SY, Wang ZJ, et al. Temporary ectopic implantation for salvage of amputated lower extremities: case reports. Microsurgery 2005;25(5):385-9.
[10] Chen ZW,Chen LE.Lower limb replantation.In Brunelli G,editor.Textbook of microsurgery.Paris:Masson;1988.p503-508.
[11] Thorlacius H, Vollmar B, Westermann S, etal. Effects of local cooling on microvascular hemodynamics and leukocyte adhesion in the striated muscle of hamsters. J Trauma, 1998, 45:715-719.
[12] Ono H, Nakagawa Y, Mizumoto S, et al. Vascular compliance and vasconstractive reactions in rat hindlimbs: compliance between storage temperature of -1?and 4?. J Reconstr Microsurg, 1997, 13:409-414.
[13] Mowlavi A, Neumeister MW, Wilhelmi BJ, et al. Local hypothermia during early reperfusion protects skeketal muscle from ischemia-reperfusion injury. Plast Reconstr Surg, 2003, 111:242-250.
[14] Kihira M, Miura T, Ishiguro N. Preservationof skeletal muscle in tissue transfers using rat hindlimbs. Plast Reconstr Surg, 1991, 88: 275-286.
[15] Norden MA, Rao VK, Southard JH. Improved preservation of rat hindlimbs with the University of Wisconsin solution and butane-dione monoxime. Plast Reconstr Surg, 1997, 100: 957-965.
[16] BeppuM, Takahashi F, Tsai TM, et al. Experimental replantation of canine forelimb afer 78.5hours of anoxia. Plast Reconstr Surg, 1989, 84: 642-648.
[17] Gordon L, Levinshon DG, Borowsky CD, et al. Imporoved preservation of skeletal muscle in amputated limbs using pulsatile hypother-mic perfusionwithUniversity ofWisconsin solution. A preliminary study. J Bone Joint Surg (Am), 1992, 74: 1358-1366.
[18] Yabe Y, Ishiguro N, ShimizuT, et al. Morphologic and metabolic study of the effect of oxygenated perfluorochemical perfusion onamputated rabbit limbs. J Reconstr Microsurg, 1994,10: 185-191.
[19] Edwards RJ, Im MJ, Hoopes JE. Effects of hyperbaric oxygen preservation on rat limb replantation: a preliminary report. Ann Plast Surg, 1991, 27:31-35.
[20] Zemmel NJ, Amis LR, Sheppard FR, et al. A temporal analysis of the effects of pressurized oxygen (HBO) on the pH of amputated muscle tissue. Ann Plast Surg, 1998, 40: 624-629.
[21] Lindgard A, Lundberg J, Rakotonirainy O,et al. Preservation of rat skeletal muscle energy metabolism by illumination. Life Sci, 2003, 72:2649-2658.
[22] Hierner R,Cedidi C,Betz AM,Berger AC.Zur standardisierung des therapeutischen Vorgehens bei der Versorgung von Amputationsund amputationsartigen Verletzungen im Unterschenkelbereich-das integrative Therapiekonzept Handchir Mikrochir Plast Chir 2002;34:277-291.
[23] Hierner R, Betz A, Pohlemann T, et al. Long-term results after lower leg replanation-Dose the result justify the risks and efforts Eur J trauma 2005;4:389-398.
Note: 1. DE-CHENG WANG, the first author, the doctoral graduate student ( 2010) in Capital Medical University Department of Orthopedics; 2. JIANG-NING WANG, the first author, the corresponding author, Capital Medical University Beijing Luhe Hospital; 3. SHOU-YU WANG, the second author, The First Hospital Affiliated to Dalian MedicalUniversity; ZHI-HONG TONG, the third author, Dalian Central Hospital; 4. LEI GAO, YE-FENG YIN, Capital Medical University Beijing Luhe Hospital; 5. YONG HAI, the corresponding author, Capital Medical University Department of Orthopedics, Beijing Chaoyang Hospital; The correspondence address of DE-CHENG WANG: , Room 2, Floor 4, Unit 5, 19 Zhong Shang Yuan, Tongzhou District, Beijing 101149; E-mail of DE-CHENG WANG: wdccjz@sina.com
|

