|
Abstract:
Introduction: Loosening has emerged as the most serious long-term complications of total hip arthroplasty with acetabular loosening being more common than femoral. Radiological assessment offers a practical method to obtain objective information about loosening.
Method: Sixty total hip replacements, in fifty four patients were performed between 1995 to 2005, using a cemented, all-polyethylene, acetabular component. The immediate post-operative and latest available radiograph of the pelvis were assessed retrospectively. Scoring of the cement-bone interface into “well-fixed” and “not well-fixed” was done. Effect of radiological scores, cup angle, age, sex and etiology on failure rates was noted. Survivorship analysis for the acetabular cup was performed.
Result: 35 hips were “Well fixed” and 25 hips were considered “Not well fixed”. 2 hips which were considered well fixed and 8 hips which were considered not well fixed had failed. The survival analysis curve showed 83% survival at 12 years. There was a significant difference in the failure rates between well-fixed and not well-fixed cups (p = 0. 0.0465), Young patients (p = 0.0318) and acetabular inclination other than neutral (p<0.0001). No significant difference was found in the radiological scores obtained according to age groups (p>0.05).
Conclusion: Early postoperative radiographs can be reliably used as an early predictor for long-term outcome. It highlights the importance of cementing technique, which is paramount in the ultimate survival of the cup.
J.Orthopaedics 2011;8(1)e7
Keywords:
Acetabular cup; Loosening; radiographic assessment
Level of evidence: IV (Case series)
Introduction:
Charnley's Cemented Hip Arthroplasty has stood the test-of-time. Femoral and acetabular loosening have emerged as the most serious long-term complications of total hip arthroplasty and the most common indications for revision, with acetabular loosening being more common than femoral1. Various cementing techniques have been developed to control radiolucency at the bone-cement interface, however aseptic loosening still remains a problem2. Improved long-term results could be obtained through the current cementing technique of the “3rd generation”, especially for cemented stems 3, 4, 5. But “3rd generation” cementing technique has not prolonged the long-term results for cemented cups equally. Here, the interface between the acetabular bone stock and the bone cement is often the weak point and therefore the main cause for aseptic cup loosening 6.
There exist clinical situations in which it becomes difficult to distinguish pain due to loosening, than from other causes7. Radiological demarcation of the acetabular cup does not always indicate clinical failure and require revision surgery8. The significance of radiolucencies around cup is still debated. Individual components of total hip replacement cannot be assessed clinically. Radiological assessment offers a practical method to obtain objective information about a particular component9. The aim of this study was to determine whether the immediate post-operative radiographs could be used to predict the longevity of Cemented Acetabular Cup
Materials and methods:
Sixty total hip replacements, in fifty four patients were performed between 1995 to 2005. All surgeries were performed by a single surgeon using a cemented, all-polyethylene, acetabular component ( Zimmer ZCA Cup) and CPT femoral stem (Zimmer, Warsaw, IN). A 22-mm femoral head was used in all cases. The femoral component was not evaluated and the present study focussed on the acetabular component. The surgical approach was posterolateral. The acetabulum was reamed down to subchondral bone. The subchondral bone was then perforated multiple times and then cleared of all the debris. The blood pressure was lowered by the anesthesiologist, and manual cementing with low viscosity cement (CMW 3) was done. Exclusion criteria included previous hip sepsis, previous ipsilateral hip surgery, use of bone grafts, any metabolic disorders and use of systemic steroids. The original cohort consisted of 36 men (40 hips) and 18 women (20 hips) with a mean age of 49 years at surgery (range, 25–70 years). Forty patients had idiopathic avascular necrosis (Ficat Type 3 and 4), ten had post-traumatic secondary osteoarthritis, four patients had rheumatoid arthritis, four had ankylosing spondylitis and two patients had healed post-tubercular osteoarthritis. The average length of follow-up was 8 years (range 2-12 years)
Radiographic Assessment
The immediate post-operative and latest available radiograph of the pelvis were assessed retrospectively. All radiographs were taken in 15 degrees on internal rotation with magnification factor of 10 % (1.10). As defined by Nunn et al9 the patient was positioned supine and the beam was centered 3 cm above the symphysis pubis with the tube at a distance of 90 cm from the plate.
Radiological demarcation of the acetabulum was noted according to the zones of DeLee and Charnley10. The acetabular angle, as defined by Murray11, was measured as the angle between the longitudinal axis and the acetabular axis. Failure was defined as a global radiolucent line of at least 1 mm in all 3 zones or any revision surgery due to loosening of the acetabular cup8.
We used the scoring system developed by Ranawat et al2 for assessment of the cement-bone interface of the immediate post-operative skiagram (Table 1).
Table 1. Scoring System
Bone-Cement Interface |
Zone I |
Zone II |
Zone III |
Perfect Interface |
1 |
1 |
1 |
Thin Lateral radiolucency |
1.5 |
1 |
1 |
Thin Radiolucency in Zone I |
2 |
1 |
1 |
Thin Radiolucency in Zone I and II |
2 |
2 |
1 |
Wide Radiolucency in Zone I |
3 |
1 |
1 |
Global Radiolucency |
3 |
3 |
3 |
Migration of the cup |
4 |
4 |
4 |
A perfect cement interface had good interdigitation of cement into underlying cancellous bone, where as a thin radiolucency was less than one mm wide and a wide radiolucency was more than one mm wide2. The scores were derived for all the three zones. These were totaled to obtain a composite score. The minimum was 3 points which indicated a perfect bone-cement interface and the maximum was 12 points which indicated migration of the acetabular component.
Accordingly, hips with a score less than or equal to 4 were considered “Well Fixed” (Fig-1) and hips with scores greater than 4 were considered “Not Well Fixed” (Fig-2 and Fig-3). However this was not a demarcation for clinical failure, but served as a red-flag to assess impending failure.
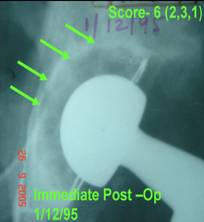 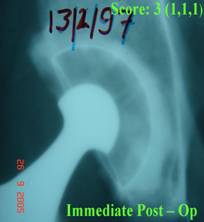 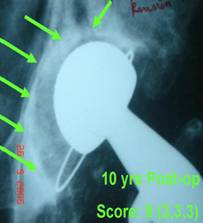
Fig 1 Well Fixed cup Fig 2 Not well fixed cup Fig3 Not well fixed cup
Immediate post op Immediate post op Loose at 10 yrs
Survivorship analysis was performed with revision for aseptic loosening and radiographic evidence of loosening as end-points. Statistical analysis was performed to verify the effect of radiological scores, cup angle, age, sex and etiology on failure rates. The associations of fixation and sex to failure rates were analysed with Fisher exact test. The difference in age of the two groups was compared with Mann Whitney test.
Cup angle was defined radiographically and the results were divided into three groups: normal (range 34º-55º), horizontal (<34º), vertical (>55º). The association of cup angle and failure rates was analysed with Pearson Chi-square test.
Null hypothesis was defined to be that there was no difference in failure rates of well fixed and not well fixed hips as defined on post-operative radiographs and immediate post-operative radiographs could not predict the long-term survival of the acetabular cup.
RESULTS:
In the present series, there were 35 Well fixed Hips (Score equal to or less than 4) and 25 hips were considered Not well fixed (Score greater than 4). With failure defined as radiographic loosening of the acetabular cup or revision for acetabular loosening, 10 hips (16.67 percent) were considered to have failed in the survival curve analysis. 2 hips which were considered well fixed and 8 hips which were considered not well fixed had failed.
Two hips have been revised, whereas eight hips await revision. Table 2 describes the distrubution of the cases and failure according to age, etiology and sex.
Table 2. Distribution of failure according to age etiology and sex
|
Group |
Total |
Failures |
Age |
|
|
|
< 20 |
0 |
0 |
|
20-30 |
3 |
1 |
|
30-40 |
8 |
5 |
|
40-50 |
19 |
3 |
|
50-60 |
15 |
0 |
|
60-70 |
14 |
1 |
|
70-80 |
1 |
0 |
Etiology |
|
|
|
Avascular Necrosis |
40 |
5 |
|
Post-traumatic secondary osteoarthritis |
10 |
2 |
|
Rheumatoid arthritis |
4 |
2 |
|
Ankylosing spondylitis |
4 |
1 |
|
Healed post-tubercular osteoarthritis |
2 |
0 |
Sex |
|
|
|
Male |
36 |
6 |
|
Female |
18 |
4 |
The survival analysis curve showed 83% survival at 12 years (Fig. 4).
Figure 4. Survivorship curve for all patients.
There was a significant difference in the failure rates between well-fixed and not well-fixed cups (p = 0.0465) (Tab. 3).
Table 3. Number of observations divided by radiological scores.
|
Radiological Scores |
|
failure |
well fixed |
not well fixed |
Total |
good |
33 |
17 |
50 |
fail |
2 |
8 |
10 |
Total |
35 |
25 |
60 |
Acetabular inclination other than neutral (p < 0.0001) was found to have a significantly higher incidence of failure (Tab. 4).
Table 4. Number of observations divided by cup alignment
|
Failure |
|
placement |
good |
Fail |
Total |
Horizontal |
0 |
2 |
2 |
Normal |
49 |
3 |
52 |
Vertical |
1 |
5 |
6 |
Total |
50 |
10 |
60 |
Difference in age between the two groups was 10 years ( p = 0.0318), patients in the failed group being significantly younger. No significant difference was however found in the radiological scores obtained according to age groups (p>0.05). Also no difference was found in the failure rates according to etiology (p>0.05).
Discussion:
There has been much improvement in the modern cementing technique with the use of cement pressurization, pulse lavage, flanged acetabular cups. Previous studies have demonstrated that cement fractures in regions of thin or incomplete cement12. To prevent these regions of thin cement, the use of polymethylmethacrylate spacers on the outside of polyethylene acetabular cups has been recommended by some13, whereas Faris et al [8], have found inconsistent results with these spacers. The use of vacuum mixing as suggested by Wixson et al14 reduces the porosity of cement to a range of 0.1%-3.4 percent and leads to a statistically significant improvement in fatigue performance. Improved cementing technique has produced a marked reduction in the rate of aseptic loosening of the femoral component but the incidence of acetabular loosening however remains variable15.
Radiological demarcation has always been a primary concern because a global radiolucent line at the bone-cement interface indicates probable prosthesis loosening16. The clinical significance of incomplete static radiolucent lines has also been much debated17. Kavanagh et al18 suggested that their presence could not be associated with clinical symptoms but the presence of radiolucent lines on early postoperative radiographs has, on the other hand, been used as an early predictor for long-term outcome. Although the criteria for acetabular loosening by Hodgkinson et al16 are widely used, terms like possible, probable and definite loosening however pose both a diagnostic and therapeutic dilemma. Moreover there is always a lag period between appearance of clinical symptoms and radiological signs.
The current study postulated that the quality of cementing as reflected in the immediate postoperative period would be a reliable marker in predicting the ultimate survival of the acetabular cup. This is strongly suggested by the significant difference in the failure rates (p<0.05) of the ‘Well-fixed” and “Not Well-fixed” cups, which also disproves the null hypothesis. It highlights the importance of cementing technique, which is paramount in the ultimate survival of the cup.
In addition to this other factors have also found to influence the survival of acetabular cups. Acetabular angle significantly influences aseptic loosening as it alters the mechanical factors acting on the cup19.Sarmiento et al20 have suggested that cups that had vertical orientation were always contained and had fewer incidences of complete cement radiolucency, however, others have suggested a more horizontal orientation21. Our study suggested a very high failure in the cups with orientation other than neutral (p<0.001).
Age of the patient was another important variable. In the current study irrespective of age all patients underwent a cemented total hip replacement, due to financial constraints. Higher rates of failure were found in the younger age group (p<0.05). Similar results have been obtained in long term studies suggesting a higher failure rate of cemented arthroplasty in younger population20, where the main cause of failure at 20 years was found to be aseptic loosening.
No significant difference was however noted in the immediate post-operative radiological scores according to age (p>0.05). This suggested that there was no bias in the two radiological groups and that the initial surgical technique was same in all patients. It can also be concluded from this that age thus played a very significant role in the subsequent survival of the cups. Young patients tend to place increased mechanical loads, with a more active life style thus influencing the survival of the acetabular cup.
Previous studies that examined the results of total hip arthroplasty performed with an acetabular component inserted with cement, at a follow-up time of 20 to 25 years, have shown revision rates for aseptic loosening of 10% to 19%, with an additional 12% to 25% of the acetabular components showing signs of loosening22, 23, 24, 25. Our study reports a survival rate of 83% at 12 years. This can be attributed to the early part of our learning curve and use of first generation cementing techniques.
A potential drawback of the study remains observer variation. Other authors have found variation in the assessment in the radiological assessment of cementing26, 27, 28 and this need to be addressed. The loosening of the femoral component is more of a mechanical process compared to that of the acetabular component which is more of a biological one. Thus, acetabular loosening in contrast to the femur tends to be a late finding, and increases dramatically after 10 years. A still longer follow-up and assessment of the actabular cup at 20 years would yield interesting results. Valle et al29 documented a higher rate of radiographic than clinical failure for the acetabular cup. On similar grounds a clinico-radiological correlation would offer more information.
Reference:
- Harkess JW. Arthroplasty of hip. In : Canale ST, Daugherty K, Jones L, Burns B, editors. Campbell's Operative Orthopaedics. 10th ed. Vol.I. Mosby: St. Louis; 2003. pp. 315-482
- Ranawat CS, Deshmukh RG, Peters LE, et al. Prediction of the long-term durability of all-polyethylene cemented sockets. Clin Orthop 1995; 317:89-105.
- Ballard WT, Callaghan JJ, Sullivan PM, Johnston RC. The results of improved cementing techniques for total hip arthroplasty in patients less than fifty years old– a ten-year follow-up-study. J Bone Joint Surg 1994;76-A:959–964
- Malchau H, Herberts P, Eisler T, Garrelick G, Soderman P. The Swedish total hip replacement register. J Bone Joint Surg 2002; 84-A Suppl 2:2–20
- Mulroy WF, Harris WH. Revision total hip arthroplasty with use of so-called second-generation cementing techniques for aseptic loosening of the femoral component. A fifteen years-average follow-up-study. J Bone Joint Surg 1996; 78-A:325–330
- Garcia-Cimbrelo E, Munuera L, Diez-Vazquez V. Long-term results of aseptic cemented Charnley revisions. J Arthroplasty 1995;10:121–131
- Berry JD. Evaluation of the painful total hip arthroplasty. In: Morrey BF. Joint replacement arthroplasty. 3rd ed. Philadelphia: Churchill Livingstone; 2003. pp. 811-823.
- Faris PM,Ritter MA, et al. The Cemented All-Polyethylene Acetabular Cup: Factors affecting survival with emphasis on the integrated polyethylene spacer: an analysis of the effect of cement spacers, cement mantle thickness, and acetabular angle on the survival of total hip arthroplasty. J Arthroplasty 2006; 21:191-198
- Nunn D, Freeman MAR, et al. The measurement of migration of the acetabular component of hip prosthesis. J Bone Joint Surg 1989; 71-B:629-631
- DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop 1976;121:20-32
- Murray DW. The definition and measurement of acetabular orientation, J Bone Joint Surg, Volume: 75-B, (1993), p. 228-232
- Jasty M, Maloney WJ, Bragdon CR, et al. The initiation of failure in cemented femoral components of hip arthroplasties, J Bone Joint Surg 1991; 73-B: 551-558
- Nelson CL, Haynes DW, Weber MJ, et al. Device and method for controlling cement thickness, Clin Orthop 1980; 151:160-164
- Wixson RL : Do we need to vacuum mix or centrifuge cement? Clin Orthop 1992; 285: 84-90
- Mulroy WF, Estok DM, Harris WH: Total Hip Arthroplasty with the so called second generation cementing techniques. A fifteen year average follow-up study. J Bone Joint Surg1995; 77-A: 1845-52
- Hodgkinson JP, Shelley P, Wroblewski BM. The correlation between the roentogenic appearance and operative findings at the bone-cement junction of the socket in Charnley low-friction arthroplasties. Clin Orthop 1988; 228: 105-9
- Kneif D, Downing MR, et al. The correlation between immediate radiolucent lines and early implant migration in cemented acetabular components. J Arthroplasty 2006;21:215-220
- Kavanagh BF, Dewitz MA, Ilstrup DM, et al. Charnley total hip arthroplasty with cement, fifteen-year result. J Bone Joint Surg Am 1989;71:1496-1503
- Ritter MA, Merrill A. The cemented acetabular component of a total hip replacement: all-polyethylene vs. metal backing, Clin Orthop, Volume: 311, (1995), p. 69-75
- Sarmiento A, Ebramzadeh E, Gogan WJ, et al. Cup containment and orientation in cemented total hip arthroplasties, J Bone Joint Surg 1990; 72-B: 996-1002
- Hirakawa K, Mitsugi N, Koshino T, et al. Effect of acetabular cup position and orientation in cemented total hip arthroplasty, Clin Orthop 2001; 388: 135-142
- Schulte KR, Callaghan JJ, Kelley SS, Johnston RC. The outcome of Charnley total hip arthroplasty with cement after a minimum twenty-year follow-up - the results of one surgeon. J Bone Joint Surg 1993; 75-A: 961-975
- Callaghan JJ, Albright JC, Goetz DD, Olejniczak JP, Johnston RC. Charnley total hip arthroplasty with cement. Minimum twenty-five-year follow-up. J Bone Joint Surg 2000;82-A:487-97.
- Callaghan JJ, Forest EE, Olejniczak JP, et al. Charnley total hip arthroplasty in patients less than fifty years old - a twenty to twenty-five-year follow-up note. J Bone Joint Surg 1998; 80-A: 704-14
- Klapach AS, Callaghan JJ, Goetz DD, et al. Charnley total hip arthroplasty with use of improved cementing techniques - a minimum twenty-year follow-up study. J Bone Joint Surg 2001, 83-A: 1840
- Kramhcoft M, Gehrchen PM, et al. Inter- and intraobserver study of radiographic assessment of cemented total hip arthroplasties. J Arthroplasty 1996;11:272-276
- Harvey EJ, Tanzer M, Bobyn JD. Femoral cement grading in total hip arthroplasty. J Arthroplasty 1998;13:396-401
- Kelly AJ, Lee MB, Wong NS, Smith EJ, Learmonth ID. Poor reproducibility in radiographic grading of femoral cementing techniques in total hip arthroplasty. J Arthroplasty 1996;11:525-8.
- Valle CJ, Kaplan K, et al. Primary total hip arthroplasty with a flanged, cemented all-polyethylene acetabular component - evaluation at a minimum of 20 years. 2004;19:23-26
|

