|
Abstract:
Carpal fractures are common but are often associated with a
difficulty in diagnosis. One reason of this is that the
configuration of the carpal bones often results in poor
radiological outcome. The pisiform is one such carpal bone that
suffers from poor radiological clarity in standard and available
special views. Delayed diagnosis may result in mistreatment and
a permanent dysfunction of the wrist. We present a new method of
obtaining radiographs of the pisiform that allows clear
depiction of the pisiform and the piso-triquetral articulation
that will aid in diagnosis of injury.
J.Orthopaedics 2010;7(1)e9
Keywords:
carpal; pisiform
Introduction:
The incidence of hand fractures in the UK is approximately 400
out of every 100000 of the population per year. Of fractures of
the hands the phalanges have been shown to be the most common
(59%) followed by the metacarpals (33%) and then the carpal
bones (8%). Pisiform fractures make up 2% of all carpal
fractures. However fractures of the pisiform are often
overlooked as they generally not visible on routine radiological
views of the wrist.
We propose taking a lateral radiograph with the wrist in
flexion, which we have found to show the pisiform and
pisi-triquetral articulation clearly and as such help in
diagnosis of bony injury.
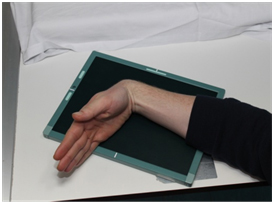
Materials and Methods:
The patient is positioned such that the forearm is in pronation
and the wrist joint is fully flexed. A radiolucent wedge may be
used to assist the patinet to achieve this position. The xray
source and plate are positioned to obtain a lateral view of the
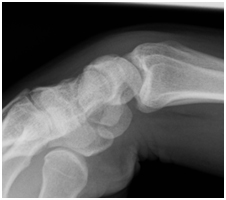
wrist in this position (fig1). The radiograph thus taken
demonstates clearly the architecture of the pisiform as well as
the pisio-triquetral joint (fig 2).
Discussion :
The pisiform lies medially, volar to the proximal row of the
carpal bones, articulating with the volar aspect of the
triquetral, which it overlies. It is a sesamoid bone, and is
attached proximally to the flexor carpi ulnaris, and distally to
the pisohamate, pisometacarpal and pisotriquetral ligaments.
Other soft tissue attachments include the abductor digiti minimi
and the transverse carpal ligament. The ulnar nerve and artery
lie immediately radial to the pisiform in Guyons canal. The
pisiform acts to increase the distance of the FCU from the
centre of rotation of the wrist, increasing the strength of the
muscle by lengthening the distance of the lever arm. Its
function is therefore similar to that of the patella in the
knee, and it also suffers from the same spectrum of disorders (fractures,
chondromalacia osteoarthritis and instability). It is most often
injured in falls on an outstretched hand
or by direct trauma. The former may cause an avulsion fracture,
while both may result in a comminuted body or transverse
fracture.
The clinical examination is invaluable in diagnosing injury to
the pisiform. The bone itself is very easily palpated on the
palmer aspect of the wrist, just distal to the distal wrist
crease, at the base of the hypothenar eminence where it also
forms a visible elevation. Examination will reveal tenderness
and swelling in this area. It is important to also examine ulnar
nerve function and wrist function as it has been shown that up
to 50% of pisiform fractures may be associated with other wrist
pathology (perilunate dislocation, distal radius fracture,
additional carpal bone fracture).
Standard radiographs of the wrist are very poor at detecting
pisiform fractures. Due to the inadequacy of AP and lateral
views of the wrist other views have been suggested- carpal
tunnel view, 30 degree supinated lateral radiograph and oblique
views. However these views are also not ideal as fractures are
not always shown. We feel that optimum clarity of the pisiform
and the piso-triquetral joint is achieved by taking a lateral
radiograph with the wrist hyperflexed as detailed above. We
surmise that this allows relaxation in the soft tissues around
the bone, namely the FCU, causing the pisiform to drop away from
its articulation with the triquetrum and in the process allowing
it to be visualised better. This view allows clear visualisation
of the pisiform enabling the clinician to verify pisiform bony
injury or disease with high reliability.
Conclusion:
Pisiform injury is an important but easily overlooked condition.
One of the reasons for this is that standard radiographic
imaging allows only poor visualisation of the pisiform. We
propose the use of a lateral view with the wrist in flexion to
allow high-quality visualisation of the pisiform and the
pisi-triquetral articulation.
Reference :
-
Hand Fractures.
Campbell, DA.
12, 2006, Surgery, Vol. 24, pp. 437-440.
-
Prevalence and distribution of hand fractures.
Van Onselen, EBH, et al.
5, 2003, Journal of Hand Surgery, Vol. 28, pp. 491-495.
-
Fractures of the hand: distribution and relatvie incidence.
Hove, LM.
1993, Scand J Plast Reconstr Surg Hand Surg, Vol. 27, pp.
317-319.
-
Forearm and wrist radiology: part 2.
Propp, DA and Chin, H.
1989, The journal of emergency medicine, Vol. 7, pp. 491-496.
-
Fractures of the carpal bones excluding the scaphoid.
MA, Shah and Viegas, SF.
2002, Journal of the american society of surgery of the hand,
Vol. 2, pp. 129-140.
-
Examination of the wristsoft tissue, joints and special
tests.
Reddy, RS and J, Compson.
2005, Current orthopaedics, Vol. 19, pp. 180-189.
-
Simon, R, Sherman, S and Koenigsknecht, SJ.
Emergency orthopaedics- the extremities. s.l. :
McGraw-Hill Professional. 2006.
-
Examination of the wristsurface anatomy of the carpal bones.
Reddy, JS and Compson, J.
2005, Current orthopaedics, Vol. 19, pp. 171-179.
-
Roentgen aspects of injuries to the pisiform bone and
pisotriquetral joint.
Vasilas, A, Grieco, V and Bartone, NF.
1960, Journal of bone and joint surgery (Am), Vol. 42, pp.
1317-1328.
|

