|
CASE REPORT |
|
Intraosseous Lipoma Of The Capitate: A Case Report |
|
Andrew P H*,Patricia L
M**,James H F**
*F. Edward Hebert School of Medicine, Uniformed Services University of the Health
Sciences, 4301 Jones Bridge Rd, Bethesda,
MD 20814
**
Department of Orthopedics, National Naval
Medical Center, 8901 Wisconsin Ave,
Bethesda, MD 20889
Address for Correspondence:
Andrew P. Hurvitz, BS, ENS, MC, USN
F. Edward Hebert School of Medicine
Uniformed Services University of the Health Sciences
4301 Jones Bridge Rd, Bethesda,
MD 20814
Email: s9ahurvitz@usuhs.mil
Phone: (323) 804-6300
|
|
Abstract:
Intraosseous lipomas are rare, benign tumors of
the bone. This report reviews the radiographic and
histopathologic findings consistent with this type of lesion
J.Orthopaedics 2008;5(4)e2
Keywords:
carpal bones; capitate; intraosseous lipoma
Introduction:
Lipomas are frequently discovered in the soft tissues.
Intraosseous lipomas, however, are considerably less common.
Despite the normal existence of fat in the marrow space, an
intraosseous lipoma is a focal growth of mature adipocytes
within the medullary cavity of bone. There is a slight male
predominance and diagnosis occurs throughout a wide age range
with a peak incidence in the forties.1,2,3 The first
case was reported in 1910 by Wehrsig4, describing an
intraosseous lipoma in the proximal fibula of a 5 year old
girl. Intraosseous lipomas occur primarily in the metaphyses of
bone, most commonly involving the long bones of the lower
extremity.1,2,3 We present a unique case of an
intraosseous lipoma discovered in the capitate of a 38 year old
man. A search of the English and Foreign literature from 1910
to present revealed 28 cases of intraosseous lipoma occurring in
the upper extremity, only one of which was described in a carpal
bone. That particular case, which also occurred in the capitate,
was reported by Baron in 1987.5
Case Report:
In May of 2006, a 38 year old right-hand
dominant male presented to a Family Practice clinic
approximately 3 weeks after falling on his outstretched left
hand. The patient reported mild pain and swelling of the left
wrist with a clicking sensation upon movement.
On physical exam, he was noted to
have tenderness to palpation at the ulnar aspect of the left
wrist, with restricted wrist motion and pain with full flexion
and extension. There was no visual deformity or palpable mass
of the left wrist. Light sensation was intact throughout both
upper extremities, and the patient had palpable, symmetric
pulses bilaterally.
Initial radiographic examination by plain
films revealed a 9mm diameter lytic lesion in the proximal pole
of the capitate, with a sclerotic, well-defined border
proximally, but poorly defined distally (Fig 1). The lesion was
presumptively diagnosed as a capitate cyst and the patient was
referred to a hand specialist for further evaluation and
definitive treatment.
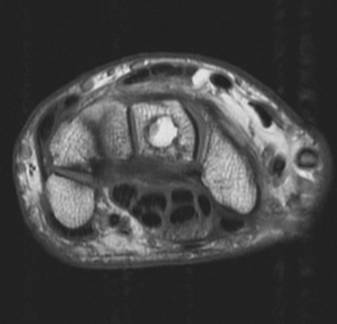
Figure 1 :
Anteroposterior radiograph of the left wrist
demonstrate a lytic lesion in the proximal pole of the capitate,
with a sclerotic, well-defined border proximally, but poorly
defined distally.
Reexamination 1 month later
confirmed earlier findings; the patient was tender over the
ulnar aspect of the left wrist, but denied any paresthesias.
Subsequent MRI revealed a well-corticated, benign-appearing
lesion with thin, sclerotic margins. Axial T1 weighted images
demonstrated a circular, hyperintense lesion within the capitate
with a focal area of hypointensity ulnarly, isointense to fluid
(Fig 2). Axial T2 fat suppressed images showed suppression of
the signal within the lesion, indicating the presence of fat.
There was also a focal area of intensity ulnarly that was
consistent with cystic degeneration (Fig 3). A diagnosis of
intraosseous lipoma was made and, after thorough discussion of
the treatment options, the patient elected for surgical excision
of the lesion.
Figure 2 :
Axial T1 weighted image demonstrates a
circular, hyperintense lesion within the capitate with a focal
area of hypointensity ulnarly, isointense to fluid.
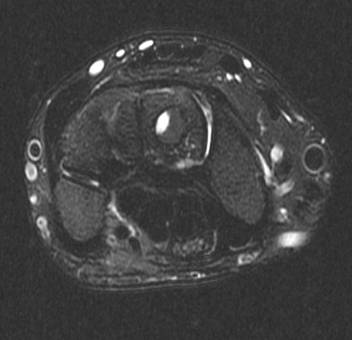
Figure 3 :
Axial T2 fat suppressed images shows
suppression of the signal within the lesion, indicating the
presence of fat. There is also a focal area of intensity
ulnarly, consistent with cystic degeneration.
Intraoperatively, the capitate was
exposed and the lesion was removed under direct vision. The
gross findings were consistent with
intraosseous lipoma, with a small focus of cystic degeneration
as seen on the MRI. The histopathology from this case is not
available for publication, however, a representative case in the
calcaneus reveals the typical features of an intraosseous lipoma,
demonstrating a proliferation of mature-appearing adipocytes
interposed with an area of ischemic ossification (Fig 4).
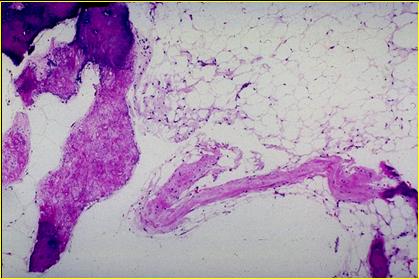
Figure 4 :Photomicrograph
of a representative intraosseous lipoma discovered in the
calcaneus, displaying a proliferation
of viable, mature-appearing adipocytes with mild degenerative
and fibrotic change and evidence of an irregular area of
ischemic ossification toward the left of the image. Courtesy of
Daniel Strum, MD; Armed Forces Institute of Pathology, Walter
Reed, Washington DC
Discussion :
Intraosseous lipomas are rare,
benign neoplasms of bone. Their incidence has previously been
reported as less than 0.1% of all bone tumors6,7,8,
however, more recent studies have suggested this value is an
underestimate.3,6,7 The reason for this
undervaluation is likely attributed to the relatively
asymptomatic nature of the lesion. These lesions are most
common in the metaphyses of long bones, particularly of the
lower extremity. A comprehensive search of the literature
revealed 28 total cases occurring in the upper extremity, only
one of which has been previously described in the capitate.5
The largest study to date was performed
by Milgram in 1988 on 61 cases of intraosseous lipomas.1
In this study, most lesions were discovered in the femur, tibia
and fibula. None of the lipomas were found in the hands or
feet, with the exception of five cases in the calcaneus.
Milgram divided intraosseous lipomas into three groups based on
their respective histology. Stage 1 lesions consist of viable
fat cells with cortical expansion; Stage 2 lesions are composed
of fat cells with areas of necrosis and calcification; Stage 3
lesions are described as having necrosis, calcification, cyst
formation, and reactive woven bone formation.
Clinically, these neoplasms may present
with localized discomfort or swelling.3,7 The
majority of cases, however, tend to be asymptomatic and are
discovered incidentally during radiographic work-up for
unrelated musculoskeletal injuries and fractures.1,2,3
In this particular case, a cystic lesion was initially described
on plain film and subsequently diagnosed as an intraosseous
lipoma, as indicated by the characteristics of the lesion on MRI.
Symptomatic patients may elect to have
intraosseous lipomas excised with subsequent bone grafting1,2,
however, surgical treatment is not a requirement. Asymptomatic
patients are encouraged to avoid surgical intervention as there
is little reported risk of malignant change.1,2,6
The rate of recurrence for these lesions is very low and has,
therefore, not been a factor in the surgical treatment of these
lesions.1,2
While the occurrence of intraosseous
lipoma is infrequent, it is important to consider this tumor in
the differential diagnosis of cystic-appearing lesions of the
carpal bones. An MRI or CT should be performed to establish the
diagnosis of intraosseous lipoma as both can accurately
demonstrate the presence of fat within a lesion.2,3,6
Reference :
1. Milgram JW.
Intraosseous Lipomas. A clinicopathologic study of 66 cases.
Clinical Orthopedics 1988; 231:277-301.
2. Milgram JW.
Intraosseous lipomas: radiologic and pathologic manifestations.
Radiology 1988;167:155-160.
3. Murphey MD,
Carroll JF, Flemming DJ, Pope TL, Gannon FH, Kransdorf MJ.
Musculoskeletal archives. AFIP Archives. Radiographics
2004;24:1433-1466.
4. Wehrsig G.
Lipom des Knochenmarks. Centralblatt fur allgemeine
Pathologie und pathologische Anatomie 1910;21: 2437.
5. Baron J,
Scharizer E. Tumors and tumor-like diseases of the carpal
bones. Handchirurgie, Mikrochirurgie, Plastische Chirurgie
1987; 19(4): 195-205.
6. Propeck T,
Bullard M, Lin J, Doi K, Martel W. Radiologic-Pathologic
correlation of intraosseous lipomas. American Journal of
Roentology 2000;175:673-678.
7. Chow L, Lee
K. Intraosseous lipoma: a clinicopathologic study of nine
cases. American Journal of Surgical Pathology 1992;
16(4):401-410.
8. Nahles G,
Schaeper F, Bier J, Klein M. An intraosseous lipoma in the
frontal bone - a case report. International Journal of Oral
and Maxillofacial Surgery 2004; 33(4):408-410.
9.
Plate A, Lee SJ, Steiner G, Posner MA. Tumorlike
Lesions and
Benign Tumors of the Hand and Wrist. Journal of American
Academy of Orthopedic Surgery 2003;11:129-141.
|
|
This is a peer reviewed paper Please cite as
: Andrew P H :
Intraosseous Lipoma Of The Capitate: A Case Report
J.Orthopaedics 2008;5(4)e2
URL:
http://www.jortho.org/2008/5/4/e2 |
|
|

