|
Abstract:
Angioleiomyomas are rare, benign, smooth
muscle tumors that are rarely found in the hand. In Butlers
review of 437 hand tumors, only one was a leiomyoma4.
We present a case of a digital angioleiomyoma that presented
with gradual enlargement and reactive bony changes of the middle
phalynx. Wide excision proved to be curative. A discussion and
review of the literature follows.
J.Orthopaedics 2008;5(2)e2
Case
Report:
A 60 year-old right-hand dominant attorney
presented with a mass on the right index finger which had been
present for several years. The patient noted that it arose
insidiously and reported no history of trauma. He sought
treatment as he felt that it had recently increased in size. He
denied any pain or recent weight loss, reported no history of
cold intolerance, and was working at the time of presentation.
On physical exam, there was
noted to be a firm mass approximately 1.5 cm in size located on
the radial volar aspect of the distal portion of the index
middle phalynx. No skin changes were appreciated. The mass was
slightly mobile and minimally tender. Sensation was normal on
the radial and ulnar aspect of the index finger, and there was
full function and range of motion of the flexor and extensor
tendons to the digit. Soft tissue swelling as well as some
reactive changes of the middle phalynx of the index finger was
appreciated on radiologic exam (Figure 1)
Differential
diagnosis at the time of examination included giant cell tumor
of tendon sheath, glomus tumor, ganglion, mucous cyst, and
lipoma.
The patient chose to have the
mass excised on an elective basis due to its recent increase in
size. The mass was excised under local anesthesia with
sedation. The mass was grossly firm and grayish in color. It
did not appear to involve the radial digital artery, vein, or
nerve. Pathologic analysis identified the mass as a completely
excised angioleiomyoma approximately 0.9x0.9x0.7 cm in size. It
stained positively for smooth muscle actin and negative for
immunostain S-100, supporting the diagnosis of angioleiomyoma
(Figure 2).


Fig. 1:Soft tissue mass and apparent sclerotic changes in
the radial and distal aspect of middle phalynx
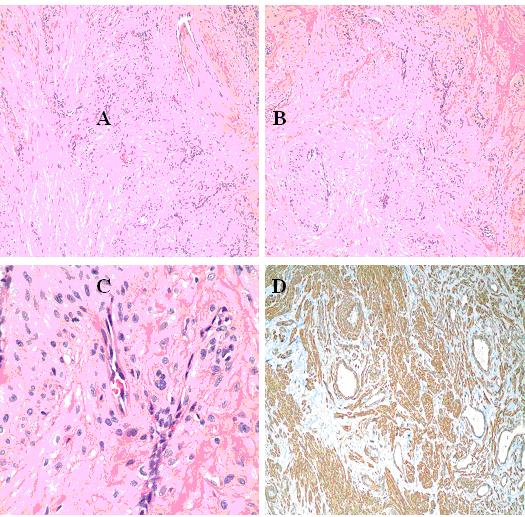
Figure 2: Microscopic and immunohistochemical
features of angioleiomyoma, solid type. A. Hematoxylin and
eosin, 40X amplification. B. Hematoxylin and eosin, 100X
amplification. C. Hematoxylin and eosin, 400X amplification. D.
Immunohistochemical stain for smooth muscle actin (200X
amplification, clone 1A4, Ventana, Tucson, AZ).
Microscopic description: The lesion is a well demarcated
nodule of smooth muscle tissue punctuated with thick-walled
vessels (Figure 2 A, B) with small partially patent lumens
(Figure 2 C). It is immunoreactive for smooth muscle antigen
(Figure 2 D)
Discussion:
Leiomyomas are benign soft tissue tumors
that are distributed wherever smooth muscle is present1.
Angioleiomyomas, a subtype of leiomyomas, are rare, benign,
smooth muscle tumors that arise from the tunical media layer of
small arteries and veins2. Angioleiomyomas may occur
in the dermis, subcutaneous fat, and fascia3.
While these
tumors may be found anywhere in the body, only rarely have they
been described in the hand. In 1937, Butler reviewed 437 hand
tumors, only one of which was a leiomyoma4. Duhig
and Ayers review of 60 angioleiomyomas revealed only 3 cases in
the hand5. In a review 85 upper extremity
angioleiomyomas at their institution, Nevaiser et al noted that
12 involved the hand6. In Hachisugas comprehensive
review of 562 cases, 56 were found to involve the hand2.
Histologically,
angioleiomyomas are divided into three subtypes: capillary or
solid (most common), venous, and cavernous (least common)2,3,7.
The most common solid type has compacted smooth muscle and many
small, slitlike vascular channels. Thick muscular walls
distinguish the venous type. In the least common cavernous
type, the vascular channels are dilated with less smooth muscle
present2. Attempts to definitively correlate
histologic subtype with clinical presentation has proven
inconclusive2,8. Some have suggested that
angioleiomyomas may in fact not be a tumor at all, but a
vascular malformation5. A recently published case
report of excision of this tumor from a digital artery with
end-to-end repair of the artery by Calle et al may support this
assertion1.
It is estimated
that approximately 50 - 60% of patients present with a chief
complaint of pain related to the mass frequently associated with
trauma or extreme cold9. This may easily be confused
with a glomus tumor, of which two-thirds are typically
associated with pain, frequently intensified by cold exposure10.
Pain is a less common presenting complaint with upper extremity
angioleiomyomas9. Many authors have found pain to be
associated with the solid subtype2,3,8. Some have
postulated that pain is due to local ischemia of the mass2.
Recently, however, nerve fibers have been visualized within
these tumors at the microscopic level11.
Angioleiomyomas
typically occur in the fourth through sixth decades2,6.
They may be anywhere from 0.5-3 cm in size, most commonly being
less than 1 cm3,6. While these tumors can be found
throughout the body, approximately 89% are reported in the
extremities, most commonly below the knee in the lower extremity2,8.
Overall angioleiomyomas are more common in females compared to
males (2.2:1)3, but there is a higher incidence of
upper extremity angioleiomyomas in males11. While
they are more frequently found on the extensor surface of the
lower extremity, these lesions appear to have a predilection for
the volar surface of the hand11. Occasionally, these
tumors may cause local bony changes12, as was found
in this case. This is likely due to local pressure effects.
Malignant degeneration is extremely uncommon, with only two
reported cases found in the literature6,13. In one
case, ray resection was necessary for local control13.
Classically, local excision of the mass is the definitive
treatment of choice.
Summary :
Angioleiomyomas
are rare, benign smooth muscle tumors that can occur anywhere in
the body. They are more common in the lower extremities, and
are rarely found in the hand. Pain is frequently present.
Malignant degeneration is extremely rare, and simple excision is
typically curative. Angioleiomyomas should be considered in the
differential diagnosis of nodular masses of the hand.
References :
- Calle SC, Eaton RG, Littler JW.
Vascular Leiomyomas in the Hand. J Hand Surg 1994
Mar;19(2):281-286
- Hachisuga T, Hashimoto H, Enjoji M.
Angioleiomyoma: A clinico-pathologic reappraisal of 562 cases.
Cancer 1984;54:126-130
- Freedman AM, Meland NB. Angioleiomyomas
of the Extremities: Report of a Case and Review of the Mayo
Clinic Experience. Plast Reconstr Surg. 1989 Feb;83(2):328-331
- Butler ED, Hamill JP, Seipel RS, de
Lorimier AA. Tumors of the Hand: A ten-year survery and report
of 437 cases. Am J Surg 1960;100:293
- Duhig JT, Ayer JP. Vascular leiomyoma:
A study of sixty cases. Arch Pathol Lab Med 1959; 68:424-430
- Neviaser RJ, Newman W. Dermal
Angiomyoma of the Upper Extremity. J Hand Surg 1977;2:271-274
- Dominguez-Cherit J, Brandariz A. Distal
Digital Angioleiomyoma: A Case Report and Review of the
Literature. Int J Dermatology 2004 Feb;42(2):141-143
- Morimoto N. Angiomyoma (Vascular
leiomyoma): A clinicopathologic study. Medical Journal of
Kagoshima University 1973;24:663-683
- Ramesh P, Annapureddy SR, Khan F,
Sutaria PD. Angioleiomyoma: A Clinical, Pathological and
Radiological Review. Int J Clin Pract 2004 Jun;58(6):587-591
- Ozdemir O, Coskunol E, Ozalp T, Ozaksar
K. Glomus tumors of the finger: a report on 60 cases. Acta
Orthop Traumatol Turc. 2003;37(3):244-248
- Lawson GM, Salter DM, Hooper G. Angioleiomyomas of the Hand. A Report of 14 Cases. J Hand Surg
(Br) 1995 Aug;20(4):479-83
- Glowack KA, Weiss AP. Vascular
Leiomyoma of the Finger Causing Bone Erosion. J Hand Surg
1995;20(6):1011-1013
- Herren DB, Zimmermann A, Buchler U.
Vascular Leiomyoma in an Index Finger Undergoing Malignant
Transformation. J Hand Surg (Br) 1995;20B(4):484-487
- Albares,MP, Belinchon I, Vergara G,
Pascual JC, Pastor E. Digital Angioleiomyoma. Int J
Dermatology 2002 Aug; 41(8):527
- Oktem F. Vascular Leiomyoma of the
Hand. Plast Reconstr Surg 2005 April;115(4):1218-1219
- Stout AP. Solitary cutaneous and
subcutaneous leiomyoma. Am J Cancer 1937;29:435-69
|

