Discussion :
The
overall incidence of pressure sores has decreased over the last
few decades due to the better understanding and availability of
preventive measures supplemented by improved nursing care.
Despite these advances, pressure sores are still a serious
problem for paraplegic patients, who are confined to a wheel
chair. It has been widely acknowledged that the results of
various available treatment procedures, in general have been
less then satisfactory.
A major
factor of rehabilitation of paraplegic patients is the
prevention of pressure sores [1], by education of the medical
and nursing staff, the patient and patients family and by
recognition and identification of high risk patients.
This
includes patients with reduced mobility, reduced or absent
sensation, loss or decrease in vasomotor control and alteration
in anatomy.
Reconstructive surgery [1] must be considered in patients not
responding to the conservative treatment:
The
problem of pressure sores [2] suffered by wheel chair bound
patients can not be approached simply with the objective of
closing ischial decubitus ulcers or by ischialectomies. The
tissue in that area must be able to stand up to the rigors of
life in a wheel chair, and if an ulcer is treated with a simple
wound closure, the problem is likely to recur.
While
there are various wound coverage procedures available [3], the
chance of recurrence exists because of insensate skin and
enormous pressure and a different approach to the problem is
required, one which confronts the underlying cause. The aim is
to restore sensation to the critical area with a sensate flap.
Various
techniques cited in the history to treat the pressure sores are:
1955
(Guttmann) - Excision of the lesion, resection of bony
prominences by following his pseudo tumour technique and
coverage of the defect with a large transposition rotation skin
flap.
1973 (Pers
and Medgyesi) Padding the sore cavity by using muscle flap
underneath the skin flap, but without neurovascular bundle
(muscle atrophies).
1979 (Dibbell
et al) Musculocutaneous flaps
The free
flap for coverage of lumbosacral region is not a straight
forward procedure mainly because of lack of the recipient
vessels. In addition the surrounding unhealthy tissue and poor
general condition of the patients makes it even more complicated
and often with not much reward.
No
amount of training can replace the timely and highly motivating
sensory experience called pain. Placement of sensory flap at the
site of pressure intimately links cause and effect. It also
provides the direct reminder of pain stimulus to the brain,
which appears to be the basis for the success of a sensory skin
flap.
The
upper quadrant flap [5] is a useful alternative in the repair of
pressure sore defects of the sacral region and also the donor
site is not disabling [5, 6]. Use of a long island flap to bring
sensation to the sacral area in young paraplegics is very
promising but the nerve bundles of T-10 and T-11 are not long
enough to reach down to the dangerous pressure areas over the
ischial tuberosities or the sacrococcygeal prominence and also a
very large decubitus ulcer could not be closed by the island
flap itself. In patients with injury level below L3-L4, a tensor
fascia lata musculocutaneous flap based on lateral cutaneous
nerve of thigh (L1, L2, and L3) can be used to provide
sensations to the defected area but not in patients with lesion
above this level.
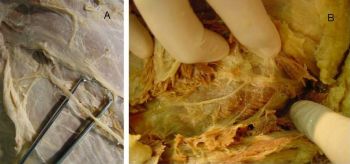
Thereby
our cadaver dissection raises a hope for a kind of sensory
reinnervation in paraplegics with lesion at the thoracolumbar
junction, in which the sensory component of the intercostals
nerves can be utilized to provide the sensation to the skin flap
covering the ischial weight bearing sores.
A few
precautions need to be taken before one embarks on the tensor
fascia lata- intercostals flap.
-
Sensory innervated tensor fascia lata flaps should be performed
only in recurrent sores when conservative treatment has failed.
-
Patient
should be intelligent enough so as to be able to relearn the
new sensations.
-
Rehabilitation must have reached an adequate level, and the
patient must be cooperative.
-
The
neurological status of the patient has to be stable.
-
As we
need the whole length of the flap to reach the ischial region
the length of the leg has to be considered.
-
Postoperatively the patient has to be kept on special pillows to
keep the ischial region free of pressure; otherwise the nerves
may get damaged.
The
procedure can be very rewarding for the patient as the formerly
anaesthetic region is converted into a sensitive area, thereby
helping the patient to sit and thereby increase sitting control
in a wheel chair [6].
Views
to ponder:
Reinnervation of the flap is a much more complicated problem.
First the surgeon must identify the one fascicle that can
reinnervate the flap (out of the 5-7 which comprise the
intercostal nerve). Then it has to be rotated down without
damage to be the donor nerve. A tension free approximation must
be performed between the donor and recipient lateral cutaneous
nerve of the thigh. For success of the reinnervated flap the
patient must be educated to use the available sensation. The
stimulus may be referred to the wrong site (donor site) -
because the cortical representation of the flap has not changed
from the intercostal area of somatosensory cortex. This appears
as a minor problem of readjustment. Once the sensory stimulus of
pain is felt by the patient, he will learn how to relieve the
discomfort felt on his thorax and make the proper postural
readjustments automatically. We would emphasize the value of
electrophysiological study for solving these problems.
Conclusion:
The
ideal candidate for this flap is a patient with paralysis at the
thoracolumbar junction level, presenting with recurrent pressure
sores due to insensitivity. Clinical application of this sensate
flap will be attempted when a suitable candidate is available,
as a large population of presenting patients have higher spinal
cord lesions. The results will be analyzed carefully to assess
the degree of return of sensation. It will also be determined
whether the addition of sensory stimulation to the flap would
contribute greatly to the long term flap viability.
List of Abbreviations
Lat: lateral, N: nerve
Competimg Interests
The authors declare that they have no competing interests.
Authors
contributions
RG did manuscript writing and literature search, TA
performed cadaver dissection and concept design, SKA performed
manuscript writing and critical revision, BKKF performed cadaver
dissection and concept design, WYI performed cadaver dissection,
SPC performed concept design and final approval of the
manuscript.
Acknowledgements
We acknowledge the help of Department of Anatomy, The University
of Hong Kong for providing the cadaver for dissection and the
necessary logistic support.
Reference :
-
Krupp S, Khunn W, Zaech GA: The use of the innervated flaps
for the closure of ischial pressure sores. Paraplegia 1983,
21(2): 119-126
http://www.medscape.com/medline/abstract/6866555
-
Sekiguchi J, Kobayashi S, Ohmori K: Free sensory and
nonsensory plantar flap transfers in the treatment of ischial
decubitus ulcers. Plast Reconstr Surg 1995, 95(1): 156-165
http://www.medscape.com/medline/abstract/7809232
-
Daniel RK, Terzis JK, Cunningham DM: Sensory skin flaps for
coverage of pressure sores in paraplegic patients. A preliminary
report. Plast Reconstr Surg 1976, 58(3): 317-328
http://www.medscape.com/medline/abstract/785501
-
Dibbell DG: Use of a long island flap to bring sensation to
the sacral area in young paraplegics. Plast Reconstr Surg 1974,
54(2): 220-223
http://www.medscape.com/medline/abstract/4602025
-
Spear SI, Kroll SS, Little JW: Bilateral upper quadrant
(intercostals) flaps: the value of protected sensation in
preventing pressure sore recurrence. Plast Reconstr Surg 1987,
80(5): 734-736
http://www.medscape.com/medline/abstract/2959975
-
Luscher NJ, de Roche R, Krupp S, Kuhn W, Zach GA: The sensory
tensor fasciae latae flap: a 9-year follow up. Ann Plast Surg
1991, 26(4): 306-310
http://www.medscape.com/medline/abstract/1872535