|
Abstract:
Glomus
tumours are uncommon tumours which most commonly present in the
fingers, where extra-digital tumours are reported as rare
occurrences. Here we present a case of a glomus tumour of the
forearm and review the presentation with the modern radiological
appearances of these tumours. We present typical MRI images of
the tumour and discuss that extra-digital sites may not be as
rare as suspected.
J.Orthopaedics 2008;5(1)e18
Keywords:
glomus tumour; forearm; MRI
Case Report:
We
report the case of a 26 year old man who presented with a 12
month history of insidious onset, discreet lump of the forearm
which became increasingly painful, especially in the cold, but
did not increase in size. On examination, the lump seemed
superficial and was exquisitely tender to palpation. There was
no overlying erythema or any other signs of local change,
inflammation or invasion.
An
MRI scan was performed to assess the swelling and to assess
depth and invasion. Figures 1 and 2 show a 1cm diameter, well
circumscribed oval lesion contained to the subcutaneous tissues,
with no abnormality of the underlying muscle. It exhibited
homogenous enhancement with contrast which is classical of a
glomus tumour (figure 2).
The
patient underwent local excision of the lump where an
encapsulated hemangiomatous lump was removed. Subsequent
histology confirmed the diagnosis of a glomus tumour with
complete margins of excision. At review appointments, the
patient was completely symptom free.
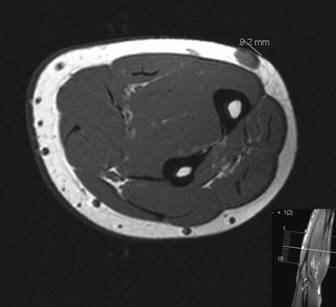
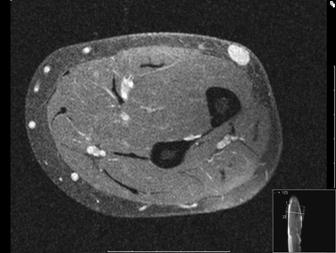
Figure
1 and 2: a well circumscribed oval lesion is found in the
subcutenous lesions (marked as 9.2mm on figure 1). Upon
administration of contrast, the lesion enhances (figure 2).
Discussion :
Glomus
tumours are benign neoplasia arising from arteriovenous
anastamoses found in the skin and subcutaneous skin of the
extremities, where they account for less than 5% of all hand
tumours. They are typically found subungally, that being on the
finger tip pulp. Symptomatically they have been classically
described as presenting with intermittent periods of pain, pain
to palpation and pain in cold conditions 1-3.
However,
glomus tumours have been reported in many extra-digital
locations of the body, including most sites of the upper and
lower limbs, the visceral organs, the lungs and trachea and the
face and nose 1-9. Although it is recognised that they are
typically associated with the fingers and hands, our patient
adds to the literature of extra-digital locations.
Whilst
ultrasound examination has been described as a traditional first
line investigation 10-12, more recently the advantages of MRI
scanning for these extra-digital tumours have replaced it 13-16.
The characteristic finding is a well-circumscribed lesion in the
subcutaneous tissues, which is enhancing on administration of
contrast 13-15, as in our patients case. MRI has the
advantages of assessing local and deep soft tissues for evidence
of invasion and other tumours, and so MRI scanning should be
considered the modern first line investigation of suspected
glomus tumours, both in the hand and extra-digitally. It can be
considered to be effective in identifying glomus tumours (sensitivity)
but not necessarily excluding them (specificity) 16.
Histology
of these tumours reveals an encapsulated lesion with no mitotic
activity. They contain an afferent arteriole and collecting
venule which are surrounded by rounded glomus cells. They may
contain smooth muscle and non-myelinated nerve endings.
In
terms of forearm tumours, pain in a well-circumscribed
subcutaneous lesion is the predominant feature 17-18 which
should arouse suspicion and prompt MRI scanning with subsequent
surgical excision. However, apt clinicians should consider the
differential diagnosis in such situations, which include
lipomas, neuroma, cysts and rarely soft tissue sarcomas. All
doctors should be familiar with the features of lumps suspicious
of malignancy: pain, deep seated lumps, size >5cm and rapid
growth 19. In contrast, glomus tumours of the forearm are often
<1cm in diameter, are superficial but are painful.
Conclusion:
Glomus
tumours are still predominately a tumour of the hand, although
they should be considered in the differential diagnosis of arm
lumps and may be more common in extra-digital locations than
suspected. The clinical presentation is often with pain, lesions
are typically less than 1cm in diameter and superficial, and
modern first line investigation is with MRI scanning. The
treatment is solely surgical excision, where the final diagnosis
is confirmed on histology.
Reference :
-
Schiefer
TK,
Parker
WL,
Anakwenze
OA et al. Extradigital glomus tumors: a 20-year
experience.
Mayo
Clin Proc.
2006 Oct;81(10):1337-44.
-
Murphy R, Rachman R. Extradigital glomus tumour as a cause of
knee pain. Plast
Reconstr Surg. 1993; 92(7): 1371-1374.
-
Amillo S, Arriola FJ, Munoz, G. Extradigital glomus tumour
causing thigh pain. J
Bone Joint Surg [Br] 1997; 79B: 104-106.
-
Okahashi K et al. Glomus tumour of the lateral aspect of the
knee joint. Arch
Orthop Trauma Surg 2004; 124(9): 636-638.
-
Mabit C, Pecout C, Araud JP. Glomus tumour in the patellar
ligament: A case report. J
Bone Joint Surg [Am] 1995; 77: 140-141.
-
Negri G, Schulte M, Mohr W. Glomus tumour with diffuse
infiltration of the quadriceps muscle: A case report. Hum
Path 1997; 28: 750-752.
-
Oztekin HH. Popliteal glomangioma mimicking baker's cyst in a
9-year-old child: an unusual location of a glomus tumour. Arthroscopy
2003; 19(7); 1-5.
-
Kapur
U,
Helenowski
M,
Zayaad
A,
Ghai
R et al. Pulmonary glomus tumor.
Ann
Diagn Pathol.
2007 Dec;11(6):457-9. Epub 2007 Jul 24.
-
Al-Ahmadie
HA,
Yilmaz
A,
Olgac
S. Glomus tumor of the kidney: a report of 3 cases
involving renal parenchyma and review of the literature.
Am
J Surg Pathol.
2007 Apr;31(4):585-91.
-
Höglund
M,
Muren
C,
Brattström
G. A statistical model for ultrasound diagnosis of
soft-tissue tumours in the hand and forearm.
Acta
Radiol.
1997 May;38(3):355-8.
-
Höglund
M,
Muren
C,
Engkvist
O. Ultrasound characteristics of five common
soft-tissue tumours in the hand and forearm.
Acta
Radiol. 1997 May;38(3):348-54.
-
Matsunaga
A,
Ochiai
T,
Abe
I et al. Subungual glomus tumour: evaluation of
ultrasound imaging in preoperative assessment.
Eur
J Dermatol.
2007 Jan-Feb;17(1):67-9. Epub 2007 Feb 27.
-
Koç
O,
Kivrak
AS,
Paksoy
Y. Subungual glomus tumour: magnetic resonance
imaging findings.
Australas
Radiol. 2007 Oct;51 Spec No.:B107-9.
-
Jewell
DJ. Case studies in the diagnosis of upper extremity
pain using magnetic resonance imaging.
J
Hand Ther. 2007 Apr-Jun;20(2):132-47.
-
Matloub
HS,
Muoneke
VN,
Prevel
CD et al. Glomus tumor imaging: use of MRI for
localization of occult lesions.
J
Hand Surg [Am].
1992 May;17(3):472-5.
-
Al-Qattan
MM,
Al-Namla
A,
Al-Thunayan
A, et al. Magnetic resonance imaging in the diagnosis
of glomus tumours of the hand.
J
Hand Surg [Br].
2005 Oct;30(5):535-40.
-
Yakubu
AA,
Mohammed
AZ,
Edino
ST,
Sheshe
AA. Glomus tumour--the report of a case in an adult
Nigerian.
Niger
J Med. 2005 Jan-Mar;14(1):97-9
-
Moor
EV,
Goldberg
I,
Westreich
M. Multiple glomus tumor: a case report and review of
the literature.
Ann
Plast Surg. 1999 Oct;43(4):436-8.
-
Johnson
CJ, Pynsent PB, Grimer RJ. Clinical features of soft
tissue sarcomas. Ann
R Coll Surg Engl. 2001 May;83(3):203-5.
|

