|
Abstract:
Giant cell tumour or
osteoclastoma is a locally osteolytic tumour which rarely
spread. It most frequently occur in the epiphysis of the distal
femur or proximal tibia, predominantly affecting skeletally
mature young adults.
We present a 16
year follow-up of a case of navicular osteoclastoma who
presented due to pulmonary lesions.
The primary site
was in the navicular. The first presentation of the patient was
at the age of 14, when he presented with shortness of breath in
a peripheral hospital. He was then diagnosed and referred to our
institution. He was treated initially with chemotherapy for
pulmonary lesions; primary site was treated with en-bloc
resection of navicular with lower pole of medial cuneiform.
There was
recurrence of pulmonary lesions three years after initial
presentation which was treated with, two stage thorocotomy.
There was no local bony recurrence.
So far there is
no agreement on how to treat patients of osteoclastoma who
present with pulmonary metastases. Our protocol to treat this
patient with chemotherapy for pulmonary lesion and excision of
the lesion at primary site proved effective, though larger
studies required to support this.
J.Orthopaedics 2007;4(4)e21
Keywords: Navicular,
Giant cell tumour, Pulmonary
metastasis, Osteoclastoma
.
Introduction:
We report a 16 year follow-up of a
case of navicular osteoclastoma, presented due to pulmonary
lesion. We discuss the course of the disease, its symptoms and
signs, treatment and final outcome.
Case Report :
13 year old boy presented in November 1987 in
another institution with sudden onset of pleuritic central chest
pain with dyspnoea on exertion and mild dyspnoea at rest. He had
complained of painless swelling in his right ankle for the last
2 years. The swelling gradually increased in size. Two months
prior to his presentation he sprained his right ankle and since
then he had complained of some discomfort in the ankle.
He was found on chest X-ray to have a
large right sided pleural effusion with bilateral multiple
pulmonary lesions with more extensive areas of abnormal density,
in the right lower lobe, posteriorly (figure 1 & 2). A foot
X-ray showed a lytic Lesion, in the right navicular bone (figure
2 & 3). A biopsy of the navicular revealed well Differentiated,
Giant cell tumour. He was transferred to our institution for
further investigation, and management.
An open lung biopsy was performed,
the histology confirmed the presence of Malignant tissue,
identical to that of the lesion in the navicular bone. The
diagnosis of Metastatic giant cell tumour (osteoclastoma) of the
navicular bone was
made.
A literature search was un-helpful
as there was no reported case at that time, of patients with
osteoclastoma, presenting with pulmonary metastases. It was
decided to treat him as malignant sarcoma and he was commenced
on chemotherapy. The agents which were used include Ifofosfamide,
Adriamycin, Vincristine, Carboplatinum, and VP16. After the
initial course of chemotherapy he developed severe neutropenia
but recovered. His pleural effusion improved and his pulmonary
lesions gradually resolved but there was no change in the size
of the primary lesion.
He received his last course of
chemotherapy, in March 1988.Because of ongoing discomfort in his
right foot, in November 1988, an en-bloc resection of right
navicular bone with lower pole of medial cuneiform was
performed.
He remained well for a period of 3
years, when he developed a recurrence of his pulmonary lesions,
bilaterally, which was evidenced by increase in the size of the
previous lesions. It was treated with two stage thorocotomy with
resection of the pulmonary Lesions. He did not receive
chemotherapy.
He was recently reviewed in
outpatients 16 years after initial presentation. He is not
reporting any problems, apart from some discomfort in the right
foot after running for 3-4 miles. Recent X-rays of right foot
showed no recurrence of primary lesion and chest radiograph
showed residual calcified nodules (figure 4) for which he has no
respiratory problems.

Figure 1:
Right side pleural effusion with bilateral pulmonary metastasis
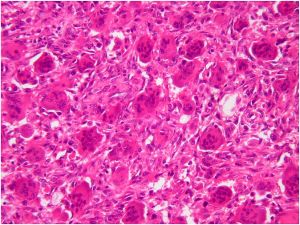
Figure 2: histology slide of pulmonary
lesion
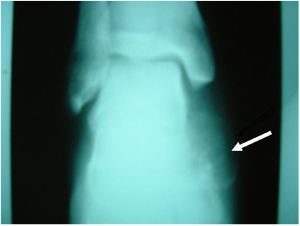
Figure 3:
Same patient with right navicular giant cell tumour
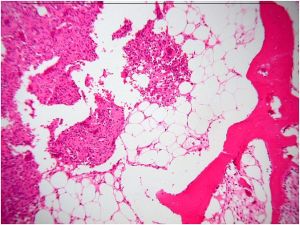
Figure 4: HISTOLGY of Navicular lesion
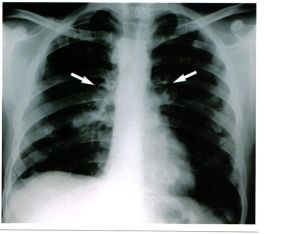
Figure 5:
Recent chest X-ray showing residual pulmonary nodules
Discussion:
Giant cell tumour has been
described as a benign tumour which gives rise to lytic lesions
in the bones and has the rare ability to spread. It affects
usually the epiphysis of the distal femur or proximal tibia,
predominantly affecting skeletally mature young adults.
Pulmonary lesions has been reported to occur in 2% of patient
with giant cell tumour1.
There are approximately 50 cases
reported of giant cell tumour with pulmonary metastases though
only a few presented with symptoms from pulmonary lesions. One
patient was treated with radiotherapy (3098 rads) for his
pulmonary lesions and resection of primary tumour2,
and another patient was treated with surgical excision of
pulmonary nodules with hemipelvectomy for his primary lesion3.
There are very few large studies
done on this topic. A study by Raphael et al4 in 1970
on 218 patients with giant cell tumour, reported the presence of
pulmonary lesions in six patients, all appeared after the
resection of primary lesion. They were treated with lobectomy
and 5 out of 6 cases were successful. Another study
by Robert et al in 19945 suggested that the overall
incidence of Spread in giant cell tumour is 0-7%.
There is so far no agreement on how
to treat patients with pulmonary metastasis and every patient is
treated differently. Recently much emphasis has been on the use
of interferon-alpha in optimizing pulmonary lesions from giant
cell tumour1.
The literature so far suggests that
the patient presented with pulmonary lesions treated with
radiotherapy showed inconsistent results with higher risk for
sarcoma transformation. Another patient who underwent surgery
had incomplete resection due to large number of
lesions.
Our protocol to treat this patient
initially with cytotoxic agents, en-bloc resection of primary
site and to treat recurrence with surgical excision proved to be
effective although, larger Studies are required to Support this.
Our patient is now 29 Years old and has no problems.
Reference :
1. Yasko A.W: Giant cell tumour of bone. Curr
Oncol Rep 2002 Nov; 4(6)520-61.
2. Cheng.J.C, Johnston.J.O: Giant
cell tumour of bone, prognosis and treatment of pulmonary
metastasis. Clin orthop.1997 ;( 338):205 214.
3. Bertoni F, Present.D and
Enneking.W.F: Giant cell tumour of bone with pulmonary
metastasis,JBJS 1985; 67-A: 890-900
4.Goldenberg Raphael R.,
Campbell.C.J, and Bonfiglio.M: Giant cell tumour of bone, an
analysis of 218 patients.JBJS 1970; 52-A (4):619-664
5. Kay.R.M, Eckardt.J.J, Seeger L.L,
Mirra J.M and Hak.D.J: Pulmonary metastasis of benign giant cell
tumour of bone, report of six cases. Clin orthop.1994 ;(
302):219-230
|

