|
J.Orthopaedics 2007;4(3)e17
Introduction:
Rhabdomyoma of soft tissue is a totally benign, non aggressive tumor, rare and originated from wrinkled muscle cells [1, 2]. This tumor is distinguished in cardiac and extracardiac localisations: the cardiac one, which is the most frequent, especially in children, and often associated to other malformations as tuberous sclerosis (50% of the cases), phacomatosis or disorders of glycogen metabolism, and the extracardiac one [3, 4, 5, 6].
Extracardiac type may be classified as adult, fetal and genital type [2]. It occurs primarily in the head and neck region, especially aerodigestive tract (pharynx, larynx and oral cavity) or soft tissues, of men and women older than 40 years, although it can occur in other places such as bladder, oesophagus, eye socket (orbits), stem and extremities. The genital type rhabdomyomas are slow growing lesions of the vagina or vulva of young middle-aged women. Fetal and adult forms can differ in relation to age: the adult one is more common at fifties, with predilection for male and the fetal one occurs in children usually less than 3 year of age. [1, 2, 4, 7, 8]
About the 110 reported cases, only one was arising in the thigh [9]. This is the second case of an extremity adult rhabdomyoma to be reported there.
We will introduce below a case of a patient with adult rhabdomyomas affecting the sartoruis muscle, image, surgical access and histopathological aspects related to the tumor as well.
Case
Report :
A
45-year-old man presented with a large right thigh mass which
had slowly grown in size over 6 months. He denied other types of
complaints, weight loss, trauma, sensory changes, or fevers.
When physically examined, he presented an 8 *
8 centimetre
firm, non tender mass in the anterior-lateral right thigh. The
mass was fixed to the deep plan and was not fixed to the
overlying skin. There were no palpable groin nodes and his pedal
pulses were present.
The
standard X-rays had shown a thickening of mild parts. (Fig A)
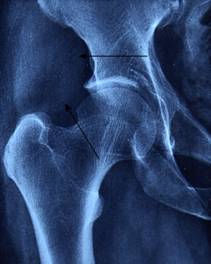
Fig
A. Radio of the hip: thickening of mild parts
In
that time, ultrasonography was requested that presented a mass
of
5 centimeter
of main line under cutanous, evoking seen its aspect a lipoma.
(Fig B)
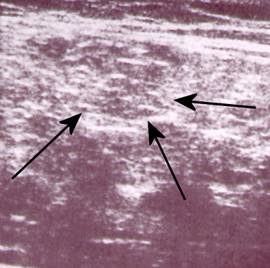
Fig
B .Echography of the tumor evoking seen its aspect
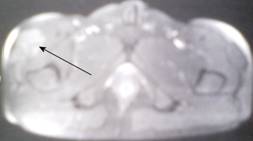
After
that, patient had an MRI, which showed: (Fig C, D)

Fig
C .IRM: formation well limited in iso signal
Fig
D. IRM: formation moderately raised after injection of the
contrast product
-
Tumefaction
corresponds to a formation limited well, in iso signal T1
and T2 compared to the muscle, measuring 6 *
4 cm
, developed within the right sartorius muscle, extended in
height, moderately raised after injection of the contrast
product in a heterogeneous way.
-
Integrity
of the under cutanous grease and the neighboring muscles
-
MRI
signal eliminates the diagnosis from a lipoma or an hematoma
==>
Tissue training of the superior 1/3 of the fleshy body of the
sartorius muscle.
The
result from fine needle aspiration puncture was not concluded.
The
patient beneficed from a biopsy altogether on the level of the
right Sartorius muscle, the sartorius muscle containing the
tumor was completely resect.
Pathologic findings:
(Fig 1,2,3,4,5)
-
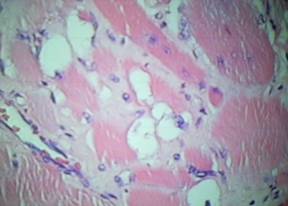
Histologically the tumor was sampled in multiple areas. Each specimen contained uniform sheets of large, round polygonal cells with eosinophil granular and focally vacuolated cytoplasm. The nuclei were large and peripherally located with dispersed chromatic, containing one or larger, pink nucleoli. No mitotic activity was identified. Tumor necrosis was absent.
-
Immunohistochemical studies performed on formali fixed, paraffin-embedded tumor tissue revealed that the tumor cells stained strongly with antibodies to desmin and myoglobin. No staining was present with antibodies to cytokeratin, S100, smooth muscle actin or vimentin.
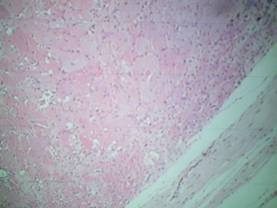
Fig1
.Low-power
view: closely packed eosinophilic polygonal cells
with a few cells having peripheral clear
vacuoles spider cells. A fibrous band
circumscribes the tumor (right)
Fig
2.
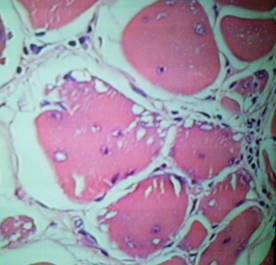
Fig
3.
The
tumor was composed of sheets of large polygonal Cells with
abundant granular, eosinophilic cytoplasm focally
vacuolated (fig 2, 3)
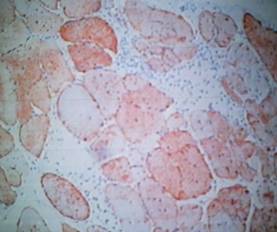
Fig
4.
Immunohistochemical
positive staining for desmin
<
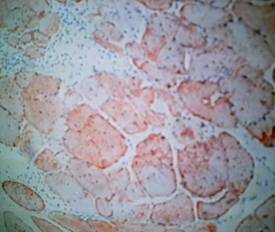
Fig
5. Immunohistochemical positive staining for
myoglobin
Discussion:
Genital rhabdomyomas are commonly present as a polypoid tumor in the vulvar and vaginal regions of young or middle-aged women [2]. Microscopically they are similar to fetal rhabdomyomas but tend to contain more differentiated myofibrils. Their pathogenesis is also unknown [9].
Adult rhabdomyomas may occur at any age [9, 14] but are more commonly found in people over the age of 40, the average age of diagnosis is 55 years, with reports ranging from 8 to 85 years, usually in the region of the head and neck [14]. The larynx, pharynx, and floor of the mouth are frequent sites of involvement. Rarely, this tumor involves the heart [15], prostate [16], mediastinum [17], orbit [18], oesophagus [19], lumbar region [27], psoas muscle [20], sternohyoid [21], trigeminal nerve [22] and stomach [3].
Magnetic resonance imaging (MRI) and computed tomography (CT) findings useful for diagnosis of Adult rhabdomyoma may be both used to determine the characteristics, extent of local involvement, and possibility of multifocality. Typically, this tumor is slightly hyper intense or iso intense to muscle on T1 and T2 weighted magnetic resonance images and demonstrates mild diffuse enhancement with gadolinium [29, 30].
Fine needle aspiration can be performed for the correct initial diagnosis to eliminate aggressive surgery [31].It is also a reliable tool especially in the oropharynx where biopsy is more difficult and hemostasis harder to achieve [9].
In the adult rhabdomyoma, cells are polygonal or ovoid with eosinophilic cytoplasm which demonstrates peripheral vacuolization resulting in a spider web appearance and focal cells with cross-striations, pathognomonic of skeletal muscle cells, and are so evident that confusion with other benign tumor is unlikely [2, 23, 24, 25, 26].
But the distinctive histopathology of the adult rhabdomyoma should not be mistaken for any type of malignant tumor.
The differential diagnosis of adult rhabdomyoma includes granular cell tumor (Abrikossoffs tumour), hibernoma and rhabdomyosarcomas but in the granular cell tumour cells lack the cross-striations and the intracellular vacuolisation; in hibernoma the vacuoles tend to be smaller, and often, areas of the tumor show obvious lipocytes; in sarcoma cells are less differentiated and they display cytoplasmic atypia and mitosis, and in rhabdomyosarcoma cells are spindle or round, showing very occasional cross-striations and atypical and pleomorphic nuclei [14,13, 28, 32].
Immunohistochemical stains can assist in proper classification if any diagnostic uncertainty remains after careful routine microscopy.
Granular cell tumors have immuno reactivity for S-100 protein but not for myogenic markers (such as actin, desmin, and myoglobin).
Hibernoma do not react with muscle immune stains, but may express S-100 protein [14, 13].
Although its histogenesis is well established, its precise nature is uncertain. Some authors suggest that it is not a true neoplasm, but a reactive tissue lesion or hamartoma due to its grade of different cells and its slow growth. Therefore, current studies showed the occurrence of clonal chromosome abnormality on tumor which supports that adult rhabdomyoma is a true neoplasm [33].
Reference :
-
kappadia
S, Meis J, Frisman DM, et al. Adult rhabdomioma of the head and
neck. Hum Pathol, 24: 608-17, 1992
-
Weiss SW, Goldblum JR. In: Weiss SW, Goldblum JR. Enzinger's and
Weiss's Soft Tissue Tumors. 4 th ed. St. Louis: Mosby: 2001
-
Di SantAgnese PA, Knowles II DM. Extracardiac rhabdomyoma: a
clinicopathologic study and review of the literature. Cancer
46:780 9, 1980
-
Rosenman D, Gertner R, Fradis M, et al. Rhabdomioma of the
larynx. J Laryngol Otol, 100:607-610, 1986
-
Liess BD, Zitsch 3rd RP, Lane R, Bickel JT. Multifocal adult
rhabdomyoma: a case report and literature review. Am J
Otolaryngol 26:2147, 2005
-
Schemen
L, Spiro R, Tuazon R. Multifocal adult rhabdomiomas of the head
and neck. Head & Neck, 14:395-400, 1992.
-
Modlin B. Rhabdomioma of the larynx. Laryngoscope, 92: 580-582,
1982
-
Favia G, Lo Muzio L, Serpico R, Maiorano E. Rhabdomyoma of the
head and neck: Clinicopathologic features of two cases. Head and
Neck 25: 7004, 2003
-
CLAIRE
T. CRONIN, MD, et al, Adult Rhabdomyoma of the Extremity: A Case
Report and Review of the Literature, HUMAN PATHOLOGY, 31: 1074 -
80, 2000
-
Fenoglio JJ, McAllister MA, Ferrans VJ: Cardiac rhabdomyoma: A
clinicopath and electron microscopic study. Am J Cardiol
38:241-251, 1976
-
Delıdes A. Multifocal adult rhabdomyoma of the head and
neck: A case report and the review of the literature. Eur Arch
Otorhinolaryngol 262:5046, 2005
-
Kapadia
SB, Meis JM, Frisman DM, Ellis GL, Heffner DK. Fetal rhabdomyoma
of the head and neck. A clinicopathologic and immunophenotypic
study of 24 cases. HUM PATHOL 24:754-765, 1993
-
Benjamin D Liess, Robert P. Zitsch, et al. Multifocal adult
rhabdomyoma: a case report and literature review. American
Journal of OtolaryngologyHead and Neck Medicine and Surgery
26: 214 217, 2005
-
Firdevs
Veziroglu , Sina Uçkan et al . Adult type rhabdomyoma in a
child. Oral Oncology EXTRA 42 : 213 216, 2006
-
Yu GH, Kussmaul WG, diSesa VJ, et al. Adult intracardiac
rhabdomyoma resembling the extracardiac variant. Hum Pathol
24:448- 51, 1993
-
Morra MN, Manson AL, Gavrell GJ. Rhabdomyoma of the prostate.
Urology 29:271- 3, 1992
-
Miller R, Kurtz SM, Powers JM. Mediastinal rhabdomyoma. Cancer
42:1983- 8, 1978
-
Knowles
DM, Jacobiec FA: Rhabdomyoma of the orbit. Am J Ophthalmol
80:1011-1018, 1975
-
Pai
GK,
Pai PK
, Kammath SM: Adult rhabdomyoma of the esophagus. J Ped Surg
22:991-992, 1987
-
Whitten RO, Benjamin DR: Rhabdomyoma of the retroperitoneum. A
report of a tumor with both adult and fetal characteristics: A
study by light and electron microscopy, histochemistry, and
immunochemistry. Cancer 59:818-824, 1987
-
Parsons
HG, Puro HE: Rhabdomyoma of skeletal muscle. Report of a case.
Am J Surg 89:1187-1190, 1955
-
Gibas S, Miettinen M: Recurrent parapharyngeal rhabdomyoma. Am J
Surg Pathol 16:721-728, 1992
-
Favia
G, Muzio LL, Serpico R and Maiora noR hEab. domyoma of the head
and neck: clinicopathologic features of two cases. Head Neck
25: 700-704, 2003
-
Enzinger
FM, Weiss SW. Soft tissue tumors. third ed. The CV Mosby
Company, pp. 43347, 1994
-
Gibas
Z, Miettinen M. Recurrent parapharyngeal rhabdomioma. Evidence
of neoplastic nature of the tumor from cytogenetic study. Am J
Surg Phatol 16: 721-8, 1992.
-
Domanski
HA, Dawinskiba S. Adult rhabdomyoma in fine needle aspirates. A
report of two cases. Acta Cytologica, 44: 223-6, 2000.
-
Piotr Ziółkowski, Bodha Raj Subedi et al. Adult
rhabdomyoma of the right lumbar region in 70-years-old woman.
Case Rep Clin Pract Rev, 5: 373-375, 2004
-
Fletcher CDM, Unni KK, Mertens F. World Health Organization
classification of tumors: pathology and genetics of tumors of
soft tissue and bone. Lyon (
France
): IARC Press 34: 142-5, 2002
-
Helmberger RC, Stringer SP, Mancuso AA. Rhabdomyoma of the
pharyngeal musculature extending into the prestyloid
parapharyngeal space. AJNR Am J Neuroradiol 17:1115- 8, 1996
-
Liang
GS, Loevner LA, Kumar P. Laryngeal rhabdomyoma involving the
paraglottic space. Am J Rad 174:1285 7, 1999
-
McGregor
DK, Krishnan B, Green L. Fine needle aspiration of adult
rhabdomyoma: A case report with the review of the literature.
Diagn Cytopathol 28:925, 2003
-
ALLEN P. BURKE, MD, CARA GATTO-WEIS et al. Adult Cellular
Rhabdomyoma of the Heart: A Report of 3 Cases, HUMAN PATHOLOGY,
33: 1092 97, 2002.
-
Gibas Z, Miettinen M. Recurrent parapharyngeal rhabdomioma.
Evidence of neoplastic nature of the tumor from cytogenetic
study. Am J Surg Phatol 16: 721-8, 1992.
|

