|
Abstract:
Ossification of
Posterior Longitudinal Ligament (OPLL) is a well recognized
cause of Cervical Spondylotic Myelopathy. However, the incidence
and management of acute traumatic spinal cord injury in a patient with
unrecognized OPLL is not well documented in literature 1. OPLL,
in itself, is a treatment challenge and
is further complicated by the setting of acute spinal
cord trauma. We present our experience in the management of a 54
year old man who became quadriplegic following a trivial fall
and was found to have severely stenotic cervical spinal canal
due to OPLL. The management strategy and the importance of a
delayed laminoplasty is emphasized.
Keywords: Ossification of Posterior Longitudinal
Ligament, quadriplegia; Cervical
Spondylotic Myelopathy; Methyl
Prednisolone; suspension
Laminoplasty.
J.Orthopaedics 2007;4(2)e9
Case report:
A 54 year old man
presented to our Emergency department, with history of
accidental fall in his home. He had facial abrasions and was
taken to a nearby hospital where the initial management was
done. He was admitted for observation. Second day, he developed
weakness of both upper and lower limbs with paresthesias
predominant in the upper limb.Then he was referred to our centre.
On examination, the patient had Grade 1/5 power of both fingers
and toes, elbow and shoulder. Hip and knee were grade zero. He
was hypotonic with absent DTRs. Anal Reflex was absent. Sensory
dulling present from C5 downwards. Patient had urinary
retention. Respiration and vitals were good.
The patient gives a history of progressive
difficulty in walking for the last 6 months for which he had
taken some form of indigenous treatment.
CT Brain was normal study.
Xray of Cervical spine showed a
significantly narrow canal with Ossified Posterior Longitudinal
Ligament (OPLL )
(Fig1)
CT Cervical Spine showed Cervical Canal
Stenosis with characteristic Posterior Logitudinal Ligament
Ossification.(Fig2)
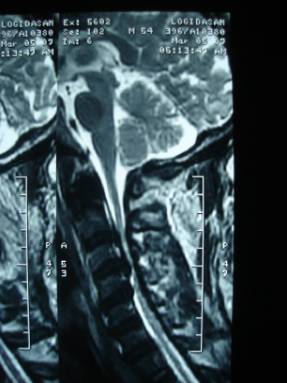
MRI showed Cervical Canal Stenosis with
diffuse form of OPLL extending from C2 to C6 vertebra producing
impingement of the Cervical Cord. Cord contusion was seen at
C4-6 levels (Fig 3 & 4)
|
|
A diagnosis of Flaccid Quadriparesis,
Spinal Shock and OPLL was made.
Patient was given Injection Methyl
Prednisolone 30mg/kg
loading dose in 15 minutes followed by a pause of 45 minutes
after which a maintenance dose of 5.4 mg/kg/hr was given
(Recommendations of NASCIS
III trial)2.. He was given Philadelphia collar. High flow
Oxygenation and hyperperfusion was given to maintain the Mean
Arterial BP at around 120mm Hg.
He was started on rigorous physiotherapy.
Third day after admission, anal reflex returned suggesting
incomplete cord injury. Progressively he had improvement of
power in both upper limbs to Gr 3/5. Knee Power increased to
Grade 3/5 bilaterally. Ankle and Toe powers remained at Gr 1/5. Both upper and lower limbs
became spastic.
He underwent Suspension Laminoplasty from
C3-C6 on the 14th day after injury.
The laminae from C3-C6 were detached enbloc
and reattached to the paraspinal
muscles. He showed progressive improvement. Over a period of 1
month, he attained near normal power of both upper limbs, and
was able to stand with support.
Discussion :
OPLL is a very
well recognized cause for Cervical Spondylotic Myelopathy3.
Although, various procedures in the form of anterior corpectomy
and fusion, posterior laminectomy or laminoplasty have been
described for management of myelopathy associated with OPLL, the
treatment protocol in a case of acute spinal cord injury in the
setting of a preexistant myelopathy due to OPLL is not clear. The study by
Koyanagi et al 1 gave varying timings for surgical
decompression.
Difficulty in
walking experienced by the patient
prior to the fall could be attributed to the myelopathy.
However, lack of space in cervical spinal canal and sudden
flexion and extension of the cervical spine during the fall
could have resulted in sudden stretch of dura against the rigid
PLL resulting in Quadriplegia. Such patients need to be managed
as a case of acute spinal cord injury with High dose Methyl
Prednisolone and Hyperoxygenation and hyperperfusion 4. The
return of anal reflex indicates a better prognosis.
In this patient ,
the decompression was done electively after 14 days because of
our previous experience which showed that early decompression in
these cases can worsen the neurology due to surgical insult to
the already compromised cord. Prospective studies have not shown any appreciable difference
in early versus late decompression in acute cervical spinal cord
injury 5.Hence, in these cases, we wait for the natural
mechanisms to halt the cord edema supplemented with other
supportive medications. Of course, there are proponents for
early decompressive surgery. However, Albert TJ et al 6 have
suggested that a spinal cord with preexistent myelopathy does
not behave in the same way as a non myelopathic cord which
sustains acute injury. They have suggested initial conservative
management followed by delayed decompression.
Laminoplasty helps to prevent or lessen the chances of similar
event occurring in the future because the canal diameter is
widened. Laminoplasty helps in posterior shifting of spinal
cord. A posterior shift of spinal cord of 3.5mm is shown to give
optimal results following laminoplasty 7.
Suspension laminoplasty
is a safer procedure for diffuse OPLL compared to anterior
procedures which are fraught with danger of injuring the dura
when the ossified ligament is adherent to the dura or when the
disease is associated with dural calcification.
Reference :
-
Koyanagi
I; Iwasaki Y; Hida K ; Imamura H ; Fujimoto S; Akino M : Acute Cervical Cord Injury associated with
Ossification of Posterior Longitudinal Ligament ; Neurosurgery
; 53 (4);887-891.
-
Bracken
MB, Shepard MJ ,Holford
TR, Leo-Summers L ,et al : Administration of
methylprednisolone for 24 or 48 hours or tirilazad mesylate
for 48 hours in the treatment of acute spinal cord injury.
Results of the Third National Acute Spinal Cord Injury
Randomized Controlled Trial. National Acute Spinal Cord
Injury Study.; JAMA 1997, May.
-
Ramani
PS ; Textbook of Cervical Spondylosis : Jaypee Publications
-
Bernhard M;
Gries A; Kremer P; Martin-Villalba A;
Prehospital management of spinal cord injuries; Anaesthetist,
2005; 54(4):357-76.
-
Vaccaro
A ; Daugherty, Reza J; Sheehan, Terrence P : Neurological outcome of Early versus Late Surgery for
Cervical Spinal Cord Injury ; Spine, 1997;, 22 (22);
2609-2613
-
Albert
TJ. Management of central cord syndrome: conservative or
delayed surgical decompression and stabilization. From the
67th annual meeting of the American Academy of Orthopaedic
Surgeons (Federation of Spine Associations, Section II);
March 18, 2000
-
Kohno K, Kumon Y, Oka Y, et
al. Evaluation of prognostic factors following expansive
laminoplasty for cervical spinal stenotic myelopathy. Surg
Neurol 1997;48:237-45.
|