|
J.Orthopaedics 2007;4(2)e28
Introduction:
Congenital
anatomical variations of the medial meniscus have been very
rarely reported in the literature.
We present a unique case of an abnormal shape and
attachment of the anterior horn of the medial meniscus not
previously described in the English literature.
Case
Report:
A
15 year old boy presented with persistent pain in his right knee
which he related to an accident which had occurred 6 years
previously. The
general practitioners letter stated that the knee locks at
times and he has difficulty in running and with playing
games. On
presentation he complained of pain on both medial and lateral
aspects of the right knee with a history of locking.
He also complained of difficulty in running and playing
any sports.
On
clinical examination the quadriceps muscle was noted to be
slightly wasted. There
was no patello-femoral discomfort.
The knee had full extension but flexion beyond 125
degrees was painful. There
was marked tenderness over both medial and lateral menisci.
McMurrays test was positive for the medial meniscus.
Lachmanns test was negative.
Radiographs did not reveal any significant abnormality.
In view of his symptoms his name was placed on the
waiting list for arthroscopy of his right knee.
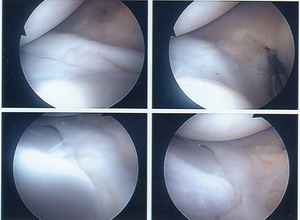
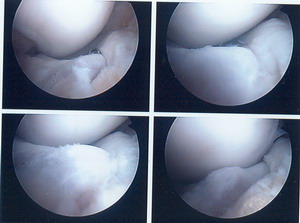
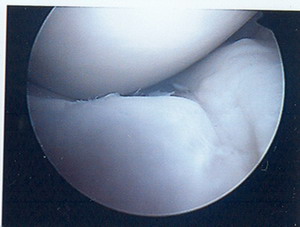
At
arthroscopy, the patello-femoral joint was found to be normal.
The anterior horn of the medial meniscus was found to be
abnormal in its shape, size (i.e. it was hypoplastic), location
and insertion (fig. 1,2,3). The size of the anterior horn
of the medial meniscus was smaller in comparison to the rest of
the medial meniscus and the attachment of the anterior horn was
not complete over the non-articular anteromedial surface of the
tibia (fig. 1, 2, 3). The anterior half of the medial
meniscus was seen to slope in its entirety towards the
anteromedial aspect of the tibia below the margins of the
articular surface with its insertion just below this (fig. 1, 2,
3). As a result in extension the medial femoral condyle
was resting directly on the articular surface of the medial
compartment of the tibia rather than the anterior horn of the
medial meniscus as is normally the case. However, the
meniscus was intact and no meniscal tear was found on probe
examination. There was a localised impingement synovitis
around the anterior part of the medial meniscus and this was
debrided. The lateral compartment was found to contain
grade 1 to 2 degenerative changes in a localised small area over
the lateral tibial plateau. There was minor fraying of the
lateral meniscal cartilage and this area was trimmed to stable
margins.
Post-operatively
the patient became asymptomatic and the portal wounds healed
well. He was
referred for out-patient physiotherapy and at the time of
reporting he remains asymptomatic.
Embryology
of the medial meniscus
During
embryological development the menisci and cruciate ligaments
appear at approximately seven weeks.
These structures are formed directly from the blastema
and not from the secondary invasion of the synovial tissue into
the joint. It is
reported that the menisci and cruciate ligaments first appear
when the crown-rump length is approximately 22 to 23 mm; even at
this early stage of development there is an even transition
between the tissues forming the menisci and that forming the
cruciate ligaments. An
anatomical study by Clarke & Ogden demonstrated that
anterior extensions from both menisci to anterior cruciate
ligaments can be present after birth1.
Discussion :
In
the normal adult knee, the anterior convex margin of the
anterior horn of the lateral meniscus is attached to the
anterior end of the medial meniscus by means of the transverse
meniscal ligament. At times, this ligament is absent. In adults,
the anterior horn of the lateral meniscus inserts on the tibia
in front of the tibial spine and its insertion is partly blended
with the anterior cruciate ligament. The anterior horn of the
medial meniscus inserts on the tibia anterior to the insertion
of the anterior cruciate ligament; it remains distinct from the
anterior cruciate ligament.
Only
a few reports of anomalous insertion of the medial meniscus
exist, and they include abnormal insertion of the medial
meniscus into the anterior cruciate ligament2, anomalous
insertion of the anterior horn of the medial meniscus into the
intercondylar notch of the femur with an absent transverse
meniscal ligament3 , and a case of an anomalous band in
continuity with the medial meniscus that extended from the
posterior horn area of the medial meniscus to insert into the
midportion of the anterior cruciate ligament4 . Other
anomalies (variants) of the medial meniscus described in the
literature include discoid variants, discoid variants associated
with a cyst, discoid medial meniscus bilaterally, absent
fixation of the transverse meniscal ligament to the tibial
plateau, buckled meniscus, hypoplasia of the anterior horn, the
posterior horn, the entire meniscus, the ACL, and anomalous
attachment of the posterior horn.
In
a morphologic study of 48 cadaveric knees, Berlet et al reported
four tibial insertion locations of the medial meniscus5: Type
I insertions were located in the flat intercondylar region of
the tibial plateau; type II occurred on the downward slope from
the medial articular plateau to the intercondylar region; type
III occurred on the anterior slope of the tibial plateau; and in
type IV there was no firm bony insertion of the anterior horn of
the medial meniscus. The occurrence for type I was reported to
be 59%; type II, 24% ; type III, 15%; and type IV, 3% .
In
an arthroscopic study of variants of the anterior horn of the
medical meniscus the authors classified medial meniscus
insertion into the following four categories6 - the ACL
(anterior cruciate ligament) type, where the anterior horn of
the medial meniscus was attached to the ACL; the transverse
ligament type, where the anterior horn of the medial meniscus
was attached to the transverse ligament; the coronary ligament
type, where the anterior horn of the medial meniscus was
attached to the coronary ligament; and the infrapatellar fold
type, where the anterior horn of the medial meniscus was
attached to the infrapatellar synovial fold.
We
report an abnormal insertion of a hypoplastic anterior horn of
the medial meniscus onto the margins of the anterior part of the
tibial plateau. It is well known that with the knee in
extension the medial femoral condyle rests on the anterior horn
of the medial meniscus as can be seen from the MRI scan(fig. 4
). In a case such as ours where there is no medial
meniscus covering the articular surface of the anterior portion
of the medial tibial plateau, in an extended knee the articular
cartilage of the medial femoral condyle rests directly on the
articular cartilage of the tibial plateau anteriorly thus
placing these portions of the articular cartilage at risk for
early degenerative changes. In our case there was
impingement synovitis in the abnormal area of the medial
meniscus and debridement of this synovitis was helpful in
relieving these symptoms.
|

|
|
Fig 4 |
Variation
in the insertion patterns of the meniscus may have other
clinical implications as some of the atypical insertions may be
unable to resist peripheral extrusion of the loaded meniscus,
placing it at risk for anterior subluxation and causing atypical
anterior knee pain. Awareness of variance in insertion
patterns and congenital anomalies may also be valuable in medial
meniscal harvest and transplantation.
Reference :
-
Clark,
C. R., and Ogden, J. A.: Development of the menisci of the
human knee joint. Morphological changes and their potential
role in childhood meniscal injury. J. Bone and Joint Surg.,
65-A:538-547, April 1983.
-
Santi
MD, Richardson AB. Bilaterally
painful anomalous insertion of the medial meniscus in a
volleyball player with Marfanoid features. Arthroscopy. 1993;9(2):217-9.
-
Shea
KG, Westin C, West J. Anomalous
insertion of the medial meniscus of the knee. A case report.
J Bone Joint Surg Am. 1995 Dec;77(12):1894-6.
-
Bhargava
A, Ferrari DA. Posterior
medial meniscus-femoral insertion into the anterior cruciate
ligament. A case report.
Clin Orthop Relat Res. 1998 Mar;(348):176-9.
-
Atay
OA, Doral MN, Aydingoz U, Leblebicioglu G. Bilateral discoid
medial menisci: association with bone changes in the tibia.
Knee Surg Sports Traumatol Arthrosc. 2001
Jul;9(4):217-20.
-
Pinar
H, Akseki D, Karaoglan O, Ozkan M, Uluc E. Bilateral discoid
medial menisci. Arthroscopy.
2000 Jan-Feb;16(1):96-101.
-
Kim
SJ, Lee YT, Kim DW. Intraarticular anatomic variants
associated with discoid meniscus in Koreans. Clin Orthop Relat Res. 1998 Nov;(356):202-7.
-
Arjun
S, Takahashi S, Tang Y, Nakane N, Yonemitsu H. MR appearance
of anomalous insertion of the medial meniscus. A case
report. Acta
Radiol. 1998 Sep;39(5):554-6.
-
Akgun
I, Heybeli N, Bagatur E, Karadeniz N.
Bilateral discoid medial menisci: an adult patient
with symmetrical radial tears in both knees.
Arthroscopy. 1998 Jul-Aug;14(5):512-7. Review.
-
Kim
SJ, Choi CH. Bilateral
complete discoid medial menisci combined with anomalous
insertion and cyst formation. Arthroscopy. 1996
Feb;12(1):112-5.
-
Kim
SJ, Kim DW, Min BH. Discoid
lateral meniscus associated with anomalous insertion of the
medial meniscus. Clin
Orthop Relat Res. 1995 Jun;(315):234-7.
-
Volkov
MV, Samoilovich EF, Serafin IuIa.
Congenital and acquired deformities of knee joint
menisci in children. Khirurgiia
(Mosk). 1994 Aug;(8):38-45. Russian.
-
Schonholtz
GJ, Koenig TM, Prince A. Bilateral discoid medial menisci: a
case report and literature review. Arthroscopy. 1993;9(3):315-7. Review.
-
Samoilovich
EF, Serafin IuIa. Development
anomalies of the menisci and transverse ligament of the
knee. Ortop
Travmatol Protez. 1991 Nov;(11):25-30. Russian.
-
Berlet
GC, Fowler PJ. The
anterior horn of the medical meniscus. An anatomic study of
its insertion. Am
J Sports Med. 1998 Jul-Aug;26(4):540-3.
-
Ohkoshi
Y, Takeuchi
T, Inoue
C, Hashimoto
T, Shigenobu
K, Yamane
S. Arthroscopic
studies of variants of the anterior horn of the medical
meniscus. Arthroscopy.
1997 Dec;13(6):725-30.
|