|
Abstract
Unicameral bone cysts in
the patella are uncommon. They are mostly asymptomatic and are
detected as an incidental finding during radiological
examination of the knee. Symptomatic cases present as anterior
knee pain or as a pathological fracture after a trivial injury.
The authors present a case of Unicameral Bone Cyst in the
patella which had resolved spontaneously following simple
fracture management of a pathological fracture of the patella.
J.Orthopaedics 2006;3(2)e8
Introduction :
Tumours of the patella are
uncommon. An extensive review of the literature by Mercuri etal
[7] had revealed only 384 cases of patellar tumours in the last
one hundred years. The common tumours are benign and include
Giant cell tumour and Chondroblastoma. Secondary metastases and
Osteosarcoma are the most frequent malignant tumours.
Unicameral bone cysts in
the patella are uncommon. Symptomatic presenting features
include anterior knee pain and pathological fracture after a
trivial injury. The management guidelines for the bone cyst in
the patella are not clearly specified in the literature.
Incidentally discovered bone cyst and that causing anterior knee
pain are managed based on bone tumour principles such as further
radiological evaluation with bone scan or magnetic resonance
imaging, biopsy for tissue diagnosis and usually undergo
surgical treatment. Operative intervention can be divided into
open and percutaneous procedures. Open methods include curettage
only, curettage combined with chemical adjuvant and bone
grafting, subtotal resection with and without bone grafting.
Percutaneous treatment technique of injecting methylprednisolone
acetate in the cyst cavity has been in vogue over the last two
decades.
Patients presenting with a
pathological fracture are usually conservatively treated based
on the principles of fracture management with immobilisation.
Such treatment results in spontaneous resolution of the cyst
with fracture healing in about 25% of the cases.
The authors present a case
of a Unicameral bone cyst of the patella presenting as a
pathological fracture which was treated successfully with simple
fracture management.
Case Report:
 A 21 year old man
presented to the accident and emergency department with
complaints of pain in the right knee following an injury when he
slipped on ice. He was able to weight bear partially after the
injury. Clinical examination of the knee showed an effusion and
restricted range of movements. Straight leg raise was painful to
perform. Radiograph of the knee showed an undisplaced
pathological fracture of the patella through a multiloculated
cystic lesion. A 21 year old man
presented to the accident and emergency department with
complaints of pain in the right knee following an injury when he
slipped on ice. He was able to weight bear partially after the
injury. Clinical examination of the knee showed an effusion and
restricted range of movements. Straight leg raise was painful to
perform. Radiograph of the knee showed an undisplaced
pathological fracture of the patella through a multiloculated
cystic lesion.
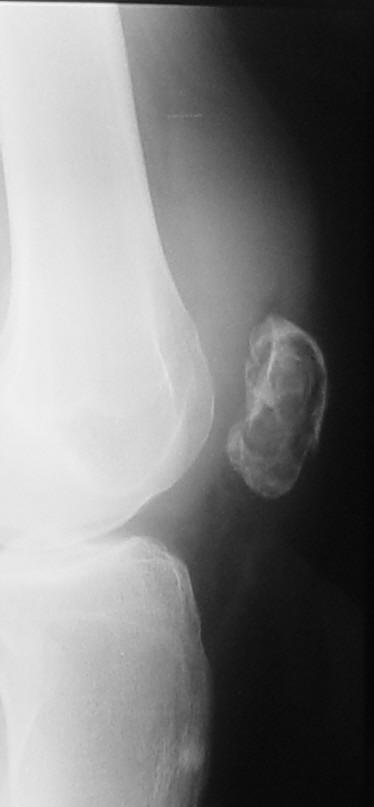 Radiological opinion confirmed the diagnosis of
the cystic lesion to be a simple bone cyst (Figure 1). Radiological opinion confirmed the diagnosis of
the cystic lesion to be a simple bone cyst (Figure 1).
The fracture was treated
conservatively with a cylinder cast for a period of six weeks.
The patient was allowed partial weight bearing during this
period. Check radiographs of the knee showed healing of the
fracture with spontaneous resolution of the cyst. A one-year
follow-up showed complete resolution of the cyst (Figure 2) and
full range of motion of the knee joint.
Discussion :
Tumours of the patella are
uncommon [3, 7]. The literature on primary tumours of patella is
very scant and majority of them are in the form of scattered
case reports and case series. Mercuri etal collected 384 cases
from a literature search from 1900 to 2000 [7]. Benign patellar
tumours are more frequent than malignant tumours. The most
common tumours included giant cell tumour and chondroblastoma,
the majority of the malignant lesions included secondary
metastasis and osteosarcoma.
Unicameral bone cyst (UBC)
was initially described by Jaffe and Liechtenstein. It is seen
predominantly during the first two decades of life, although not
necessarily limited to these age groups. It is characterised
pathologically by a thin-walled cavity developing most often
within the metaphysis of a long tubular bone, closely adjacent
to the growth plate and appearing to migrate away from the
growth plate as it matures. A UBC may appear in virtually any
bone, but typically, it is found in either the proximal humerus
or proximal femur. Most of the patients with a UBC are
asymptomatic and diagnosed as an incidental finding during
radiological examination. Symptomatic presentation is usually
due to a pathological fracture following a trivial incident.
Anterior knee pain has been recognised as a presenting feature
[6].
Radiologically, the lesion
is characterized by a large, well-localized radiolucent
expansile lesion which may be multiloculated. The differential
diagnosis includes aneurysmal bone cyst, giant cell tumour,
fibrous dysplasia and enchondroma [5].
The treatment of
unicameral bone cyst is variable. Nonoperative treatment is
usually followed for presentation with pathological fracture
when fracture immobilisation and watchful waiting results in
obliteration of the cyst. The success rates of such treatment
have been variable and reports of approximately 25% of cases
resulting in spontaneous healing have been quoted, although not
all authors recommend this treatment option [6].
Surgical treatment can be
divided into open and percutaneous procedures. Open methods of
treatment include curettage only, curettage combined with
chemical adjuvants and bone grafting, subtotal resection with
and without bone grafting. Percutaneous treatment technique of
injecting methylprednisolone acetate in the cyst cavity has been
in vogue over the last two decades. Other reported
percuataneous injections include alcohol based fibrosing agent,
autologous bone marrow and injection of demineralised bone
matrix.
Bone cyst in the patella
is uncommon. Only anecdotal case reports could be found in the
literature [1,2,4,8,9 and 10]. The treatment of patellar bone
cyst has been variable [1, 6]. Non operative in the form of
fracture management and watchful waiting was followed for
pathological fracture and operative methods of curettage and
autologous bone grafting or patellectomy were performed for
presentations with anterior knee pain with or without swelling.
In the present case, a
conservative approach of management was adopted which resulted
in the spontaneous obliteration of the cyst cavity with healing
of the fracture.
Reference :
-
Cole WH.
Primary Tumours of Patella. J Bone Joint Surg 1925; 23:
637-654.
-
Deepak
Chaudhary, Naval Bhatia, Abrar Ahmed, Chopra R K. Unicameral
bone cyst of the Patella. Orthopaedics 2000; 12: 1285-1286.
-
Ferguson PC,
Griffin AM, Bell RS. Primary Patellar Tumours. Clin Orthop
1997; 336: 199-204.
-
Jucker C,
Cuneo L. Juvenile solitary bone cysts of the patella.
Presentation of a case report. Ann Radiol Diagn (Bologna).
1962; 35: 192-194.
-
Linda M Parman,
Mark D Murphey. Alphabet Soup: Cystic Lesions of Bone.
Seminars in Musculoskeletal Radiology 2000; 4(1): 89-101
-
Masaki Chigira,
Susumu Maehara, Satoru Arita, Ehchi Udagawa. The aetiology and
treatment of simple bone cysts. J Bone Joint Surg [Br] 1983;
65B: 633-636.
-
Mercuri M,
Casadei R. Patellar Tumours. Clin Orthop 2001; 389: 35-46.
-
Saglik Y, Ucar
DH, Yildiz HY, Dogan M. Unicameral bone cyst of the patella. A
case report. Int Orthop 1995; 19(5): 280.281.
-
Schultz E,
Greenspan A. Case report 378: Simple bone cyst. Skeletal
Radiol 1986; 15(5): 405-407.
-
Weintroub S,
Salama R, Baratz M, Papo I, Weissman SL. Unicameral bone cyst
of the Patella. Clin Orthop 1979; 140: 158-161.
|

