|
ABSTRACT
We have
retrospectively reviewed the medical records of one hundred and
sixty five patients with the clinical diagnosis of ankle
fracture. In eighty-six of them, we found in the distal fibula
three different types of oblique fractures. On the basis of the
location of the line of fracture and its spatial orientation,
our patients could be grouped as follows: In 23% (20/ 86) of the
x-rays, the oblique line of fracture begun below the syndesmosis
(Type A) . Type B fracture (at the syndesmosis) was present in
70% (60/86). The line of fracture was above the syndesmosis in
7% (6/86) of the patients (Type C). These findings clearly
indicate that, in the distal fibula the line of fracture can be
located below ,at level or above the syndesmosis and still have
an oblique spatial orientation.
KEY WORDS: Weber Classification, Fractures.
Ankle, Stability criteria
J.Orthopaedics 2004;1(3)e2
INTRODUCTION.
The oblique fractures of the distal part of
the fibula, without medial lesion, are the most common ankle
fracture. They exhibited an oblique fracture line, began
anteriorly at level or below the fibula anterior tubercle and
below at level or over the syndesmosis. The fracture line goes
toward hind in approximately a third of diameter of the bone and
it spreads in anteriorposterior and distal proximal in
relationship to the old axis of the fibula in angle of some 45
grades approached with or without rupture of the inferior
tibiofibular ligament (Schaffer and Manoli,1987).Have received
several denominations such as: supination - external rotation
stage 2 (SE-II) (Lauge Hansen 1954),B (Weber 1966) ,B1 (Müller
et al 1990) and oblique short (Harper 1983,1995) . This study is
intended to review this type of fracture in The Universitary
Hospital of Los Andes (Merida.Venezuela).
MATERIAL AND METHODS.
We found that the mean age of the patients
with short fibular fracture was 37.1 years (range 18 to 87);
there were 49 men and 37 women. Between 20 to 49 years old, the
men to women ratio was 1.6 (42/26), and in more than 50 years
old the woman to men ratio was 1.6(11/7) .On the basis we have
retrospectively reviewed the medical records of 165 patients
who were seen at the University of Los Andes Hospital in Merida
Venezuela, between 1989 and 1994, with the clinical diagnosis of
ankle fracture. Eightysix(52%) of them had an oblique trace
fracture in the distal fibula without medial lesion. The x-rays
were taken in standard views (Bohlin 1961). In all of them, there
was evidence of a closed epiphysis. We classified the
ankle fractures according to the site of the fibula injury,
within the distal syndesmosis, and the likelihood of displacement
of the fracture segments. (Type A : horizontal fracture located a
the level or below the syndesmosis, Type B : fracture that begins
at the level of the syndesmosis and goes obliquely and
posteriorly, Type C : an oblique fracture above the syndesmosis (Weber
1966,Müller et al 1991). Particular attention was paid to the
spatial orientation of the line of fracture and to the stability
of the ankle mortise (Table 1). On the basis of the latter, the
fractures were considered to be stable or unstable. In the
lateral views, we also measured the length of the fracture line.
RESULTS.
According to Lauge- Hansens
expriment(1954,1959) ,Weber s(1966) and Müller et al(1991)
ankle fracture classification is whether location of the line of
fracture, sex, stability criterions, and the long of its spatial
orientation, our patients could be grouped as follows: In 23%
(20/ 86)of the x-rays, the oblique line of fracture begun below
the syndesmosis and58% (14/24) of the sex masculine (Type A)
(Figure 1). Type B fracture was present in 70% (60/86) and
prevailed in the female sex in a 52% (27/52)(Figure 2). The line
of fracture was above the syndesmosis in 7% (6/86) and they
affected both sex (Type C) (Figure 3). .We considered to be
stable 91%of the fractures, in the C Type the 83% were
stable (Table 2). The line of fracture was long oblique or spiral
in its spatial orientation in 38% of the xrays (Figure 4), the
remaining of the x-rays showed that only 62% of the lines of
fracture were short oblique (Table 2).
Table 1
|
Site |
Criteria |
X-Ray |
|
Medial clear space |
Less than 4mm |
Mortice view |
|
Syndesmosis A |
Less than 5mm |
AP view |
|
Syndesmosis B |
Less than 10mm |
AP view |
|
Syndesmosis C |
Less than 1mm |
Mortice view |
|
Lateral Malleolus |
Less than 2mm |
Mortice view |
|
Talar tilt |
Less than 2mm |
Mortice view |
CRITERIONS OF STABILITY (De Souza and
Forester 1974, JOY
ET AL 1974, LEEDS AND EHRLICH 1984,
PETTRONE ET AL
1983, PHILLIPS ET AL 1985, RAMSEY AND
HAMILTON 1976)
Table 2
|
Type |
Stable |
Unstable |
Short Oblique |
Long Oblique |
|
A |
20 |
15 |
05 |
00 |
|
B |
53 |
07 |
35 |
25 |
|
C |
05 |
01 |
03 |
03 |
|
Total |
78 |
23 |
43 |
28 |
Relationship between criterions of
stability and longitude of the fracture trace
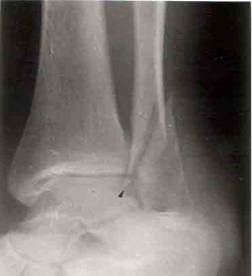
Figure 1
In this mortise view the arrow indicates
that the long oblique fracture begins below the
syndesmosis and the fracture is therefore stable

Figure 2
In this patient the short oblique line of
the fracture (arrow) is at the level of the fibular
anterior tubercle and again the fracture is stable

Figure 3
The short oblique trace of the fracture is
above them syndesmosis (thin arrow), and instability
of the fracture is obvious (a medial clear of more than 4
mm is present. (Thick arrow).

Figure 4
Spiral oblique long fracture of the fibula,
a medial clear of more than 4 mm (thick arrow) and
displacement of the lateral malleolus are present however
the syndesmosis is preserved (thin arrow)
DISCUSSION
The isolated fractures of the distal fibula
have been considered the most frequent fracture of the ankle (Harper
1995) and they represent between 10% at 40% of all of them (Lindjô 1981, Ryd
and Bengtsson 1992). Mainline the male sex but with more fracture in
women older than 50 years old (Benger et al 1986, Daly et al 1987, Desouza et al
1985). All of this is similar to our result in the present paper.
the oblique distal fibular fracture is
always located at the level , or above the tibiofibular syndesmosis. In the
present study, we found that 28% of the oblique traces were below the syndesmosis.
Earlier clinical and experimental studies support our findings (Cedell
(1967),Pankovich (1979) Schaffer and Manoli (1987) and Stiehl (1992). In these
investigations, the line of fracture begun below the level of the articular line
and may occur without any rupture of the anterior tibiofibular ligament.
The fracture trace, short oblique or a
longer or spiral, does not have a clinical decisive importance, since most of
these fractures are stable and for this reason the criterions of treatment
are not altered for the longitude of trace.
Another very important aspect of Webers
(1966) and Müller et al (1991) classification concerns the stability of
Type C fractures. We found that, 83% of oblique fractures above the syndesmosis
with no medial injury, were stable as previously reported by De Souza and
Forester(1974), Monk (1969) and Pankovich (1978, 1979).
The fact a group of these fractures like
unclassifiable in the Weber andMüller et al system could exist , the short
fibular fracture below the syndesmosis and the C and C1 stable, and
the difficulties than we and another(11,16) met with this
classifications , have stimulate us to prefer that the ankle fractures should be managed
according to the stability criterions (4,5,6,13,20,21,22). With them all the
signal flaws are eliminated from the other classifications and they have the
great advantage that they allow to value in short and long term, the outputs
and any therapeutic utilised plan.
REFERENCES
1.- Benger U, Johnell O, Redlund-Johnell I.
Epidemiology of ankle fractures1950-1980. Increasing incidence and elderly
women. Acta Orthop Scand57:35-38. 1986
2.- Bohlin, H .The Fibula and its
Relationships to the Tibia and Talus inInjuries of the Ankle Due to Forced
External Rotation. Acta Radiol ;56 :439-448. 1961
3.- Cedell, C.A . Supination-outward
rotation injuries of the ankle. A clinical and roentogenological study with special
reference of the operative trratment. Acta Orthop Scand ; (Suppl.110) 1967.
4.- Daffner, Richard H . Ankle Trauma.
Radiol Clin of North Amer ;28(2) 395-421. 1990
5.- Daly PJ, Fitzgerald RH, Melton LJ,
Ilstrup DM . Epidemiology of ankle fractures in Rochester Minnesota. Acta
Orthop Scand; 58: 544-5511987
6.- De Souza Dias L, Forester T.P.
Traumatic Lesion of the Ankle Joint. ClinOrthop ;100 :219-224. 1974
7.- Joy G, Patzakis MJ, Harvey JP . Specify
evaluation of the reduction of severe ankle fractures. Techniques and
correlation with end results. J Bone Joint Surg;56A: 979-985. 1974
8.- Harper,M.C . An Anatomic Study of the
Short Oblique Fracture of the Distal Fibula and Ankle Stability. Foot and
Ankle ; 4 :23-29. 1983
9.- Harper MC .The short oblique fractures
of the distal fibula without medial injury: An assessment of Ankle
displacement. Foot and Ankle Int ; 16(4):181-187. 1995
10.- Hughes JL, Weber H, Willenegger H,
Kuner H . Evaluation of ankle fractures: non-operative and operative
treatment. Orthop Clin of NA ; 138:111-117. 1979
11.-Kennedy J.G, Johson S.M, Collins A.L,
Dallo Vedoba P, McManus W.F,Hynes D.M, Walsh M.G, Stephens M.M. An
evaluation of the Weberclassification of ankle fractures. Injury..
29(8):577-80. 1998
12.- Lauge-Hansen . Fracture of the
ankle. Combined experimental-surgical and experimental-roentgenelogic
investigations. Arch Surg ; 60: 957-970.1959
13.- Lauge-Hansen N .Fracture of the ankle
III.Genetic roentgenelogic diagnosis of fractures of the ankle.Amer J
Roentgenol ; 71: 456-464. 1954
14.- Leeds HC, Ehrlich MG .Instability of
the distal tibiofibular syndesmosisafter bimalleolar and trimalleolar ankle
fractures.J Bone Joint Surg ; 66A: 490-496. 1984
15.- Lindsjo U. Operative treatment of
ankle fracture dislocations.Acta OrthopScand (Suppl.189).52:36. 1981
16.- Lindsjo U.Classification of ankle
fractures: The Lauge-Hansen or AOsystem. Clin Orthop..199:12-16. 1985
17- Monk C.J. Injuries of the Tibio fibular
Ligaments. J Bone Joint Surg; 51B:330-336, 1969
18.-Müller M, Allgower M, Schneider R,
Willenegger H : Manual of Internal Fixation. New York, Springer Verlag. 1979
19.-Nielsen JO, Dons-Jensen H, Sorensen HT:
Lauge-Hansen Classification of Malleolar Fractures.An Assessment of the
Reproductibility in 118 Cases. Acta Orthop Scand ; 61 (5): 385-391.
1990
20.-Pankovich, A .Fracture of the Fibula
Proximal to Distal Tibiofibular Syndesmosis. J Bone Joint Surg ; 60(A) :
221-227. 1978
21.-Pankovich, A.Fracture of the Fibula at
the Distal Tibiofibularsyndesmosis.Clin.Orthop;143: 138-145. 1979
22.-Pettrone FA, Gail M, Pee D, et al
.Quantitative Criteria for Prediction of Results after Displaced Fractures of Ankle. J Bone Joint Surg ; 65A: 667-662.1983
23.-Phillips WA, Schwartz HS, Keller CS et
al .Prospective RandomisedStudy of the Management of Severe Ankle
Fractures.J Bone Joint Surg; 67(A): 67-73. 1985
24.-Ramsey PL, Hamilton W .Changes in
Tibiotalar Area in Contact Causedby Lateral Talar Shift.J Bone Joint Surg
;58A: 356-362. 1976
25.-Schaffer J.J, Manoli A . The
Antigliding Plate for Distal Fibular Fixation J.Bone Joint Surg ;69 A :596 -604. 1987
26.-Stiehl J.B, Skrade D.A, Johnson R.P .
Exprimentally Produced Ankle Fractures in Autopsy Specimens. Clin Orthop;
285 : 244-249. 1992
27.-Weber, B.G . Die Verletzungen gives
oberen sprunggelenks. Bern, HansHuber 1966.
28.-Wilson FC .The Pathogenesis and
Treatment of Ankle Fractures:Classification. Instr.Course Lect ; Chapter
8.Vol39: 79. 1990
|

