Address for Correspondence:
Yusuke Mochizuki, M.D.
Department of Orthopedic Surgery, Nippon Medical School
1-1-5 Sendagi, Bunkyo-ku, Tokyo 113-8603, Japan
Phone:+81-3-3822-2131
Email:yusuke-mochizuki@nms.ac.jp
Abstract:
We present three cases with ligamentum flavum (LF) hematoma. Two men cases (54 and 70 years old) and one woman case (69 years old) developed low back pain and thigh pain. Magnetic resonance imaging (MRI) revealed a space occupying lesion in the epidural space at lumbar level that was continuous with ligamentum flavum. Their symptoms were immediately reduced after removal of the hematoma and there has not been any recurrence to date. The ligamentum flavum hematoma is a relatively rare and the cause has not yet been determined. The differential diagnoses include neoplasm, lumbar spinal canal stenosis or lumbar disc herniation. We reports the courses, results of imaging studies, surgical findings and a review of the literature.
J.Orthopaedics 2011;8(4)e11
Keywords:
Ligamentum flavum hematoma; Magnetic Resonance Imaging; Surgical treatment.
Introduction:
The LF hematoma is a relatively rare entity and the cause has not yet been determined. Several authors have reported that these lesions are caused by minor traumas, while others attribute the cause to insufficiency of coagulation function or to anticoagulative therapy. When LF hematomas occur in the lumbar spine, the presentation is often low back and/or leg pain accompanied by various neurological deficits. As the symptoms resemble other lumbar diseases, LF hematoma of the lumbar spine needs to be distinguished from lumbar spinal stenosis. Due to the wide spread availability of magnetic resonance imaging (MRI), the number of reports concerning LF hematoma has been increasing. Recently, we encountered three cases that involved the lumbar spine. This report describes the courses, results of imaging studies, surgical findings and a review of the literature.
Legend to figures and tables
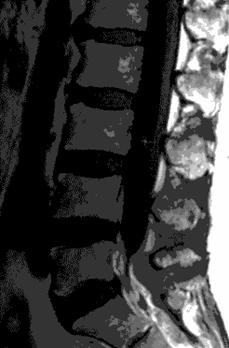 
Fig 1a (T1) Fig 1b (T2)
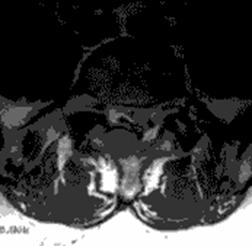 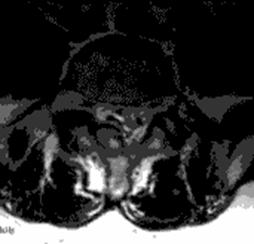
Fig 1c (T1) Fig 1d (T2)
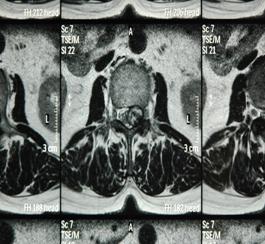
Fig 1. Sagittal (a,b) and axial (c,d) T1, T2-weighted MRI showing a space occupying lesion in the epidural space at L5/S1 level. The lesion was iso-hyperintense on T1-weighted images (T1W) and mixed pattern of intensities on T2-weighted (T2W) imaging sequences.
 
2a (T1) 2b (T2)
2c (T1) 2d (T2)
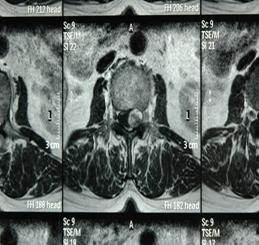
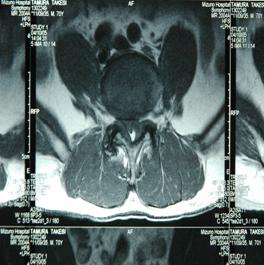
Fig 2. Sagittal (a,b) and axial (c,d) T1, T2-weighted MRI showing a space occupying lesion in the epidural space at L2/3 level. The lesion was 13mm in diameter and showed mixed intensities on both T1 and T2 weighted images.
 
3a (T1) 3b (T2)
3c (T1) 3d (T2)
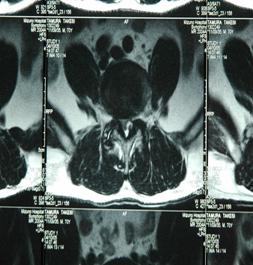
Fig 3. Sagittal (a,b) and axial (c,d) T1, T2-weighted MRI showing a space occupying lesion in the epidural space at L4/5 level. The lesion was iso-hypointense on TlW and iso-hyperintense on T2W images.
Fig 4. Incidence cases by age from the literature.Fig 5. Incidence cases by lumbar level from the literature.Fig 6. Incidence cases by chief complaint from the literature.Fig 7. Incidence cases by findings on physical examination from the literature.
Case1
A 54-year-old man developed sudden onset of pain and numbness of the right thigh and pubic region in January 2008. Although the symptom transiently decreased, the same symptoms returned the next evening. He saw a doctor and was prescribed some NSAIDs, although severe pain persisted after taking this medication. The patient consulted our hospital the next day. He had no history of trauma or lumbar surgery.
The patient was obese with a BMI of 32.3. He complained of pain and numbness on his right buttock and the bilateral lower limbs and limped due to leg pain. On neurological examination, he demonstrated weakness of the right hamstrings (MMT 4/5) and slight hypesthesia on the right foot sole. Ankle jerk was depressed on the right side. Results of routine laboratory studies were within the normal range except for slight liver dysfunction. X rays showed spondylolysis in the fifth lumbar spine. MRI demonstrated a space occupying lesion in the epidural space at L5/S1 level. The lesion was iso-hyperintense on T1-weighted (T1W) images and showed a mixed pattern of intensities on T2-weighted (T2W) imaging sequences (Figure 1).
The surgery was performed under a preoperative diagnosis whether LF hematoma or epidural tumor. The L5 lamina was removed and the L5/S1 ligamentum flavum was incised, and then drainage of a bluish black hematoma was observed. The hematoma existed between the superficial and deep layers of LF and the epidural space. The dural tube and the S1 nerve root were compressed by the hematoma. The source vessel of the hemorrhage could not be recognized. After excision of the hematoma, the L5 lamina was replaced in the original position and fixed with screws. Pain and numbness were reduced immediately after surgery. The neurologic deficit recovered and bone union was obtained. There has not been any recurrence for two years.
Case 2
A 69-year-old woman fell down and was bruised on the low back in September 2009. One month later, low back and left thigh pain developed. Because the pain did not diminish, she consulted our hospital. She had cardiac disease due to hypertension and atrial fibrillation, and had been treated with antithrombocytic agents. She complained of pain on the front aspect of the left thigh that worsened while walking. She demonstrated intermittent claudication after walking 50 meters. There was no disturbance of sensation, muscle strength or deep tendon reflexes. Routine laboratory studies, including coagulation profiles, were within the normal range. X-rays of the lumbar spine showed spondylosis. MRI demonstrated a space occupying lesion in the epidural space at L2/3 level. The lesion was 13mm in diameter and showed mixed intensities on both T1 and T2 weighted images (Figure 2).
The surgery was performed under a preoperative diagnosis of LF hematoma. After performing L2 laminectomy, brownish masses and thick hematoma were observed within thinned layers of left ligamentum flavum and the surfaces of the ligaments were pigmented with hemoglobin. The hematoma and ipsilateral LF were removed totally and the lamina was replaced and secured with polyethylene tapes. Her symptoms resolved quickly, and there has not been any recurrence for one year to date.
Case 3.
A 70-year-old man experienced low back and left thigh pain in July 2005. Pain was increased by walking and decreased with sitting, intermittent claudication was observed with after walking 50 meters. He had no preceding history of trauma or lumbar surgery. A local doctor performed conservative treatment under a diagnosis of lumbar spinal stenosis, though his symptoms did not respond to the therapy. Four months later, he was referred to our hospital. He had hypertension and benign prostatic hypertrophy and had been taking calcium blockers. Neurological examination did not show any abnormalities. Results of routine laboratory studies, including coagulation profiles, were all within the normal ranges. Plain X-ray film showed Meyerding grade I spondylolisthesis at L4. MRI demonstrated a space occupying lesion in the epidural space at L4/5 level. The lesion was iso-hypointense on TlW and iso-hyperintense on T2W images (Figure 3).
Surgery was performed under preoperative diagnosis of epidural tumor. L4 laminectomy was performed. A hematoma was identified between the layers of ligamentum flavum at L4/5 level. The dura was compressed by the hematoma. The hematoma was excised along with the LF and decompression of the dura was achieved. A posterolateral fusion with instrumentation was performed between L4 and L5. Leg pain was reduced immediately after surgery and there has not been any recurrence to date.
Discussions.
Sweasey1 et al reported the first case of a LF hematoma in 1992. To our knowledge, 127 cases of LF hematoma including our three cases have been reported in the literature. Seventy-eight (61%) cases were male and 49 (39 %) cases were female. The mean age at onset was 67.9 years old (29 -89 years old), and they occurred most frequently during the eighth decade (Figure 4). The pathogenesis of the hematoma has not yet been determined. Episodes of minor trauma such as fall or lifting a heavy load were noted in 25 cases. Complicated disease such as coagulation factor deficiency was reported in one case2 and liver cirrhosis in another case. Although there were twenty-one cases of hypertension, its correlation to LF hematoma was unclear. A drug trigger was suspected in 8 patients taking anti-coagulant and 3 patients taking antithrombocytic agent. There were no obvious causes in more than half of the cases. The lumbar spine was involved in more than 90% of cases, followed by 7 thoracic cases (6%) and 5 cervical cases (4%). In the lumbar spine cases, 45 (36%) involved L4/5 and 28 (23%) involved L3/4 (Figure 5).
The clinical signs of LF hematoma in the lumbar spine are similar to those of lumbar spinal stenosis. The most common symptom reported was leg pain followed by low back pain, neurogenic claudication and leg numbness. Bowel bladder incontinence was rare and reported in only 0.9% of the cases (Figure 6). Muscle weakness or sensory disturbance was observed in more than half of the cases on physical examination. Tension signs were noted in 15% of the cases (Figure 7).
Diagnosis of LF hematomas was made on MRI in most of the cases, and it should be differentiated from space occupying lesions in the epidural space, such as neoplasms and intervertebral disc herniations. The characteristic MRI findings are 1) posterolateral location in the epidural region, 2) connection between the LF and the mass, 3) change of MRI signal intensities with the time course3, 4. MRI signal intensity of the hematoma was documented in several radiological reports5, 6, 7. Generally, MRI signals of a hematoma change with changes in the chemical properties of hemoglobin in the hematoma8. However, radiological findings of a hematoma are considered to be influenced not only by changes in its chemical properties but also by other causes such as repetition of the bleeding, variations in the histological distribution of the serous component and its fibrous portion and the capsule9, 10. Therefore, it is often not easy to make a correct diagnosis of a LF hematoma preoperatively. In our series, MRI intensities varied significantly among the subjects and the variation was considered due to differences in the time of presentation. Several reports refer to the usefulness of MRI with contrast enhancement for the differential diagnosis of LF hematoma from epidural neoplasm. It should be important to take the age of hematoma into account when making a diagnosis of this disease.
As treatment, surgeries were performed for the all of the reported cases, though only 20 % of them underwent surgery within one month after onset and the source of hemorrhage has not yet been identified. In general, the vascular supply for the ligamentum flavum is scarce and it is often difficult for the source vessel of the hemorrhage to be recognized. Kitahama11 described the blood vessels of the ligamentum flavum as a tomentum of fine blood vessels. It receives arterial supply from epidural branches of the segmental arteries and its venous outflow drains to the posterior radicular vein via the internal vertebral venous plexus. Kashiwagi12 et al made a histologic observation of the LF on a specimen collected during lumbar spinal surgery. They report that there were many foci of small granulation tissue accompanied by rich capillaries and histiocytes and abundant proliferation of collagen fibers especially in specimens collected from patients more than fifty years old. Concerning the mechanism of hematoma formation partial tears occurred in degenerative ligamentum flavum might lead to intraligametary bleeding13.
Conclusion
We reported three cases of the LF hematoma and reviewed the literature. As MRI signal intensities of the LF hematoma change during the time course, when we encounter an epidural mass with heterogeneous intensities on MRI, LF hematoma should be considered in the differential diagnosis.
Reference :
- Sweasey TA, Coester HC, Rawal H, Blavas M, McGuillicuddy JE. Ligamentum flavum hematoma. Report of two cases. J Neurosurg 1992; 76:534-537.
- Takami M, Yamada H, Kubota S, Tamaki T. Ligamentum Flavum Hematoma in the Lumbar Spine in a patient with Congenital Factor ⅩⅠ Deficiency. Spine & spinal cord 2007;20(8):945-948
- Hasegawa A, Ichimura S, Hoki N, Aikawa D, Takahashi M, Hasegawa M, Satomi K. Ligamentum flavum hematoma in the lumbar spine with epidural hematoma. A case report. Kanto journal of orthopedics and traumatology 2009(2):37-40.
- Hiramatsu T, Fujimoto Y, Kanazawa T, Okuda A, Chikarada T, Nishikawa K. The operative case of ligamentum flavum hematoma in the lumbar spine. The Central Japan Journal of Orthopaedic Surgery & Traumatology 2009; 52: 555-556.
- Bradley WG Jr. MR appearance of hemorrhage in the brain. Radiology 1993; 189: 15-26.
- Kaplan PA, Dussault R, Helms CA, et al. Musculoskeletal MRI. Philadelphia (PA): Saunders; 2001: 71.
- Zeev V. Maizlin, Jason R. Shewchuk, Jason J. Clement. Easy Ways to Remember the Progression of MRI Signal Intensity Changes of Intracranial Hemorrhage. Canadian Association of Radiologists Journal 2009; 60: 88-90.
- Sebastian S, Florian S, Martin W, Roland K. Case reports. A Rare Cause of Radicular Complaints. Ligamentum Flavum Hematoma. Clinical Orthopaedics and Related Research 2006 Number 443: 337-341.
- Mizuno J, Nakagawa H, Inoue T, Hashizume Y. Ligamentum Flavum Hematoma in the Lumbar Spine. Neurol Med Chir (Tokyo) 2005; 45: 212-215.
- Wada H, Kishiba Y, Kinugasa T, Ainoya T, Aoto K. Comparatively uncommon case of ligamentum flavum hematoma in the lumbar spine. Kanto journal of orthopedics and traumatology 2010 (2);53:413-416.
- Kitahama Y, Hanakita J, Tamiya A, Fukao S, Minami M. Acute and Chronic Hematoma in the Lumbar Flavum -Two Cases Reports-. Spinal Surgery 2006;20(3): 193-199.
- Kashiwagi K. Histological Changes of the Lumbar Ligamentum Flavum with Age. Journal of the Japanese Orthopaedics Association 1993;67: 221-229.
- Cruz-Conde R, Berjano P, Buitron Z. Ligamentum flavum hematoma presenting as progressive root compression in the lumbar spine. Spine 1995; 20:1506-1509.
|

