Chong Mei Fong*, Chng Tun Wang**,Liza Sharmini Ahmad Tajudin**, Saravanan Shanmugam***, Zulkifli Atan***, Ramanathan Ramiah***
*Department of Ophthalmology, Hospital Raja Permaisuri Bainun, Ipoh, Malaysia
**Department of Ophthalmology, Universiti Sains Malaysia, Malaysia
***Department of Orthopaedics, Hospital Raja Permaisuri Bainun, Ipoh, Malaysia |
Address for Correspondence:
Ch’ng Tun Wang
Department of Ophthalmology,
Universiti Sains Malaysia Hoapital,
Malaysia.
Email: tunwang@yahoo.com
Abstract:
We describe a rare case of postoperative visual loss in a patient with a precious eye following a laminoplasty of cervical spine for severe spinal stenosis of C3-C6 under general anaesthesia. During surgery, patient was positioned prone supported by a horse shoe shaped head rest with eyes covered with eye pads.
J.Orthopaedics 2011;8(4)e1
Keywords:
Central retinal artery occlusion; Spinal surgery; horse shoe shaped head rest
Introduction:
Postoperative visual loss in non-ocular surgery is a rare complication. The incidence range from 0.0008% to 1% for all types of non-ocular surgery. [1-3] The risk of postoperative blindness shown to be highest following spine surgery compare to other non-ocular surgery. [1, 4] The incidence of post operative visual loss following spine surgery varies between 0.094%[5] and 0.2%.[6]
Case Presentation:
A 57 years old gentleman whom suffered from stiffness of fingers and his lower limbs complicated with difficulty in walking and restriction in doing daily activity underwent laminoplasty of cervical spine for severe spinal stenosis of C3-C6 under general anaesthesia. During spinal surgery of 2 hour duration the patient was positioned prone with the head supported by a horse shoe shaped head rest. The eyes were covered with eye pads and plaster. Intraoperative was uneventful. Vital sign monitoring during surgery recorded a regular blood pressure and heart rate by anaesthetist. The intraoperative blood loss was minimal of 450ml. Post operatively, patient complained sudden onset painless blurring of vision on his right eye. Visual acuity was hand movement. Right cataract surgery was done 9 years ago with good vision post cataract removal. The exact preoperative vision of right eye was uncertain. However, it was the better eye patient had been depending on for daily living as the left eye was blind since childhood. Ocular examination of the right eye revealed positive relative afferent pupillary defect (RAPD). The intraocular pressure (IOP) was within normal limits of 16. Examination of right eye under slit lamp shown the intraocular lens was stable with quiet anterior chamber. Ocular fundus examination revolved pink optic disc, attenuated arteries and cherry red spot at macula with area of patchy whitening suggestive of central retinal artery occlusion (CRAO)(Figure 1). This eye shows attenuated retinal artery at 4th month of follow up (Figure 2). Unfortunately, Left visual acuity was poor (6/60). Fundus examination of contralateral left eye shows optic atrophy (Figure 3). Systemic and neurological examinations were normal.
Patient was immediately advised for ocular massage. Prompt treatment of oral Acetazolamide 125mg twice per day and Latanoprost topical anti-glaucoma eye drop were started. Further investigation by Ultrasound Doppler of carotid artery and heart echocardiography shows normal study. Post operative full blood count was normal.

Figure 1: Right eye: Pink disc, attenuated arteries with cherry red spot at macula with area of patchy whitening suggestive of Central Retinal Artery Occlusion (CRAO)
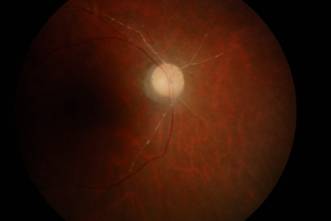
Figure 2: Right eye: 4 month post CRAO. Attenuated retinal artery.
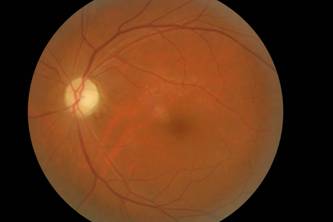
Figure 3: Left eye: Optic atrophy.
Discussion :
Central retinal artery occlusion (CRAO) occurs following trauma, embolic, thrombotic or vasospasm episodes. The overall incidence of postoperative CRAO was found to be 0.001%.[5] CRAO presents with a positive relative papillary defect, cherry red spots on macula, white ground grass appearance of retina and attenuated arterioles with preserved choriocappilaries. Literature review shows that majority of cases are unilateral and associated with post operative periocular swelling and erythema.[1] In our case, patient had postoperative CRAO with concurrent contralateral eye optic atrophy. We were unsure the exact cause of the contralateral eye optic atrophy. Childhood trauma and post inflammation of optic nerve may be the cause of optic atrophy.
Hypotension, peripheral vascular disease and anaemia are the risk factors to develop postoperative visual loss.[5] The surgery for our patient was uneventful, and no episodes of intraoperative hypotension and no history of peripheral vascular disease. Patient was non-anaemic preoperative and intraoperative blood loss was minimum.
The pathogenesis of CRAO is thought to be cause by external ocular compression.[7] The main cause for this patient to develop CRAO, postoperatively , was thought to be the external ocular compression. Extensive pressure on the globe may raise intraocular pressure (IOP) above the systolic blood pressure (SBP) leading to retinal ischemia. [8] Our patient was positioned prone with the head supported by a horse shoe shaped head rest. The eyes were covered with eye pads and plaster. Even though this horse shoe shaped head support had been used for all the previous similar surgeries without causing any complications, possibility of improper positioning of the patients eyes compressing on the head rest might have caused the blindness. Majority of post operative CRAO cases were in prone position or supine position with excessive ocular pressure secondary to anaesthetic mask.[8] Similar complication has been reported by Grossman et al which horseshoe headrest were used.[8] In a study by Hunt et al confirmed that IOP rises significantly in anesthetized, prone patient compare to patient in supine position.[9] Both external compression and rise of IOP during anaesthesia contribute to retinal ischemia.
Time of surgery is also a contributing factor. This patient undergone 2 hour of spine surgery. A study by Heyrah has shown that retina can tolerate pressure induced ischemia for approximately 95 minutes and still recover. It suffer permanent ischemia after 105 minutes of ischemia in an experiment in Rhesus monkeys.[10]
Conclusion:
As conclusion, postoperative visual loss is a devastating perioperative complication. Increase awareness of occurrence of this devastating complication is essential to surgeon, anaesthesiologists, ophthalmologist and the most important preoperative discussion with patient regarding the risk of postoperative visual loss. Proper preoperative counselling and visual assessment is essential especially in patient with precious eye. In this case, patient is legally blind with the contralateral optic atrophic left eye became the better eye. This patient had lost his left eye sight during childhood and unfortunately he lost his right eye sight while trying to resolve his cervical myelopathy symptoms.
Consent:
Informed consent was obtained from the patient for publication of this case report and any accompanying images.
Competing interests:
The authors declare that they have no competing interests.
Authors’ contribution:
CMF is the ophthalmologist manages the patient. SS, ZA and RR are the orthopaedic surgeons in charge of the patient. CTW and LSAT wrote the original report and performed a literature review. All authors have read and approved the final manuscript.
Reference :
1. Berg, K.T., A.R. Harrison, and M.S. Lee, Perioperative visual loss in ocular and nonocular surgery. Clinical Ophthalmology (Auckland, NZ). 4: p. 531.
2. Roth, S., et al., Eye Injuries after Nonocular Surgery: A Study of 60,965 Anesthetics from 1988 to 1992. Anesthesiology, 1996. 85(5): p. 1020-1027.
3. Warner, M.E., et al., The frequency of perioperative vision loss. Anesthesia & Analgesia, 2001. 93(6): p. 1417.
4. Shen, Y., M. Drum, and S. Roth, The prevalence of perioperative visual loss in the United States: a 10-year study from 1996 to 2005 of spinal, orthopedic, cardiac, and general surgery. Anesthesia & Analgesia, 2009. 109(5): p. 1534.
5. Patil, C.G., et al., Visual loss after spine surgery: a population-based study. Spine, 2008. 33(13): p. 1491.
6. Stevens, W.R., et al., Ophthalmic complications after spinal surgery. Spine, 1997.22(12): p. 1319.
7. Hollenhorst, R.W., H.J. Svien, and C.F. Benoit, Unilateral blindness occurring during anesthesia for neurosurgical operations. Archives of Ophthalmology, 1954. 52(6): p. 819.
8. Grossman, W. and W.T. Ward, Central retinal artery occlusion after scoliosis surgery with a horseshoe headrest: case report and literature review. Spine, 1993. 18(9): p. 1226.
9. Hunt, K., et al., Changes in intraocular pressure in anesthetized prone patients. Journal of Neurosurgical Anesthesiology, 2004. 16(4): p. 287.
10. Hayreh, S., H. Kolder, and T. Weingeist, Central retinal artery occlusion and retinal tolerance time. Ophthalmology, 1980. 87(1): p. 75. |

