Address for Correspondence
Shariff R
Alder Hey Children's NHS Foundation Trust
West Derby
Liverpool L12 2AP,United Kingdom
Abstract
Procedures commonly used to correct knee flexion deformities include hamstring release, anterior femoral hemiepiphyseodesis and femoral extension osteotomies. The latter procedure can cause neurovascular complications. Femoral stapling procedures are not popular because of a theoretical risk of permanent physeal closure. We report our results following the use of a 2 hole tension band plate (8-plate; Orthofix SRL, Verona, Italy). This uses guided growth in the distal femoral physis to achieve gradual correction. A consecutive series 25 of patients (46 limbs) who underwent an anterior distal femoral hemi-epiphyseodesis using the 8-plate technique between April of 2008 and August 2010 were studied. Preoperative and post operative flexion deformity was measured using a goniometer and serial radiographs.Mean age - 11.04 years (range between 4- 16), Mean follow up - 16.2 months (range 6 – 34), Mean correction achieved – 21.5 degrees (range 5 – 40),Mean correction per month - 2.05 degrees. This is a simple technique with few complications to date. Patients in our series have shown promising results, with sustained gradual correction to date. Based on our experience with the 8-plate we make recommendations which we hope will benefit surgeons using this technique.:
J.Orthopaedics 2011;8(3)e11
Keywords:
growth principle
Introduction:
Flexion contractures of the knee joint are frequently encountered in children with cerebral palsy and other neuromuscular conditions. Anterior knee pain is a common complaint and in extreme cases stress fractures of the patella can occur. Crouch gait, short stride length and decreased cadence further compromise the ambulatory status of these patients. The aims of treatment are to improve mobility in walkers and to allow non-walkers to perform weight-bearing transfers with less effort. The established treatment options for knee flexion contractures in children include hamstring release, femoral extension osteotomy with or without patellar tendon advancement and anterior distal femoral hemi-epiphysiodesis using staples. However risks such as neurovascular compromise, physeal arrest and recurrence limit their utility. We report our results following the use of a 2 hole tension band plate (8-plate; Orthofix SRL, Verona, Italy) in a series of 25 children (46 limbs) with knee flexion contractures secondary to cerebral palsy and other neuromuscular conditions. The 8-plate is a 2-hole extra-periosteal non-locking plate, which relies on the tension band principle to achieve sustained and gradual correction of the deformity. This technique has been described by Stevens et al for correction of frontal plane deformities1 and more recently for the correction of fixed flexion deformities in patients with cerebral palsy, spina bifida and unknown neuromuscular conditions amongst other causes2.
Material and Methods :
We reviewed a consecutive series of 25 children with fixed flexion contractures of the knee between April 2008 and August 2010 that underwent anterior distal femoral hemi-epiphysiodesis using the 8-plate. There were 23 children with cerebral palsy and 2 children had Arthrogryposis. A total of 46 limbs were operated upon. The pre-operative and postoperative knee flexion contracture(KFC) in degrees was recorded using a goniometer by the senior authors either in the clinic and in cases where significant additional hamstring spasticity/ shortening was noted, the measurements were carried out under general anaesthesia. The knee flexion contracture was rounded off to the nearest 5 degrees to accommodate variations due to inter-observer error and diurnal variations in muscle tone. Antero-posterior and lateral radiographs were obtained pre-operatively in all cases to confirm the presence of open growth plates and to record concomitant abnormalities such as patella alta. All complications were recorded. Paired t-Test was undertaken to assess the correction achieved.
The operative technique has previously been described in a paper by Dr Peter Stevens, the originator of this technique1.
Results :
Table 1: Summary of results
Total number of patients |
25 |
Sex |
Males |
19 |
Females |
6 |
Total number of operated limbs |
46 |
Mean age |
11.04 (Range: 4 – 16) |
Mean follow up |
16.2 months (Range: 3 – 34) |
Mean correction achieved |
21.52º |
Mean correction achieved per month |
2.05º |
Mean deformity (Patients with KFC less than 400) |
Mean deformity (Patients with KFC greater than 400) |
Pre-operative |
Post-operative |
Pre-operative |
Post-operative |
24.2 |
7.96 |
54.25 |
31.75 |
A paired ‘t’ test showed that the amount of correction was highly significant (p value < 0.001).
When patients were sub-divided into 2 categories namely those with a knee flexion contracture greater than or equal to 40 degrees and those with contractures less than 40 degrees, we found a significant improvement in the correction achieved in the latter group (Pearson’s Chi Squared test x2 =11.12, p<0.001)
Table 2: Patient Characteristics
Patient |
Sex |
Age |
Diagnosis |
Operated side |
Pre op deformity |
Post op deformity |
Follow up months |
Result |
1 |
M |
11 |
CP |
Bilateral |
20 |
5 |
16 |
Discharged |
2 |
M |
16 |
CP |
Right |
30 |
0 |
24 |
Discharged |
3 |
F |
12 |
CP |
Bilateral |
60 (bil) |
Rt – 30
Lt – 20 |
19 |
Under F/U |
4 |
M |
14 |
CP |
Bilateral |
Rt – 30
Lt – 60 |
Rt – 30
Lt – 45 |
24 |
Discharged |
5 |
M |
9 |
Arthrogryposis |
Bilateral |
90 (bil) |
60 (bil) |
24 |
Under F/U |
6 |
M |
12 |
CP |
Bilateral |
40 (bil) |
10 (bil) |
12 |
Under F/U |
7 |
M |
15 |
CP |
Bilateral |
30 (bil) |
30 (bil) |
25 |
Under F/U |
8 |
F |
12 |
CP |
Bilateral |
40 (bil) |
5 (bil) |
19 |
Discharged |
9 |
M |
14 |
CP |
Bilateral |
30 (bil) |
10 (bil) |
13 |
Under F/U |
10 |
M |
15 |
CP |
Right |
30 |
10 |
34 |
Discharged |
11 |
F |
12 |
CP |
Bilateral |
40 (bil) |
15 (bil) |
25 |
|
12 |
M |
15 |
CP |
Bilateral |
Rt – 35
Lt – 25 |
Rt – 15
Lt – 20 |
8 |
Under F/U |
13 |
F |
4 |
CP |
Right |
25 |
0 |
27 |
Under F/U |
14 |
F |
8 |
CP |
Bilateral |
10 (bil) |
0 (bil) |
6 |
Under F/U |
15 |
M |
15 |
CP |
Bilateral |
Rt – 45
Lt – 40 |
10 (bil) |
5 |
Under F/U |
16 |
M |
13 |
CP |
Bilateral |
20 (bil) |
Rt – 0
Lt – 5 |
29 |
Under F/U |
17 |
M |
6 |
Arthrogryposis |
Bilateral |
90 (bil) |
Rt – 70
Lt – 60 |
11 |
Under F/U |
18 |
M |
12 |
CP |
Bilateral |
15 (bil) |
0 (bil) |
3 |
Under F/U |
|
19 |
M |
10 |
CP |
Bilateral |
70 (bil) |
45 (bil) |
15 |
Under F/U |
|
20 |
M |
10 |
CP |
Bilateral |
30 (bil) |
Rt – 5
Lt – 10 |
15 |
Under F/U |
|
21 |
F |
5 |
CP |
Bilateral |
Rt – 20
Lt – 10 |
0 (bil) |
10 |
Metalwork removed |
|
22 |
M |
8 |
CP |
Bilateral |
Rt – 40
Lt - 30 |
Rt – 10
Lt – 5 |
9 |
Under F/U |
|
23 |
M |
10 |
CP |
Bilateral |
25 (bil) |
Rt – 0
Lt – 5 |
6 |
Under F/U |
|
24 |
M |
9 |
CP |
Bilateral |
30 (bil) |
10 (bil) |
4 |
Under F/U |
|
25 |
F |
9 |
CP |
Right |
40 |
10 |
22 |
Under F/U |
|
The mean correction per month across both categories was calculated to be 2.060.
Koshino index is the ratio of the patella-tibia distance to the femur-tibia distance versus the knee flexion angle at which the radiograph was obtained. Koshino index is used to accurately measure the patellar height in varying degrees of knee flexion3. There was no change in the Koshino index 3 between pre- and post-operative values (p>0.05).
No premature physeal closure was seen in any of the patients in this study.
There was one complication to date, failure of the distal screw at the screw head-to-shaft interface.
Discussion :
Knee flexion contractures commonly cause a significant impairment in functional abilities in a number of neuromuscular conditions. A combination of overactive spastic knee flexors (hamstrings) and weak knee extensors (quadriceps) aided by gravity contribute to development of this problem4,5. Measures to reduce spasticity such as intrathecal baclofen or botulinum toxin are effective if employed before fixed contractures develop. In the presence of a fixed contracture; correction in walkers helps maintain ambulation. In non-walkers, it helps to maintain standing in frames and improve the ability of children to stand for transfers. This aids carer giving and in some instances can determine whether the child can be cared for at home6.
Various techniques both operative and non-operative have been described in the literature for the correction of knee flexion contractures. In planning an intervention, the degree of motor involvement in the lower limbs should be assessed as this is the principle factor that determines ambulatory potential7.
Conservative methods such as hinged splints8, wedge plasters9,10 and physical therapy are used for the correction of modest contractures in the region of 20 degrees. In cerebral palsy, the progression of contractures with growth frequently necessitates the use of operative intervention11. Hughes et al used wedge plasters in patients with poliomyelitis. The disadvantage of this technique was the need for several months of plaster immobilization, risk of neurovascular compromise in severe contractures and iatrogenic supracondylar fractures of the femur 9,12.
Operative interventions such as supracondylar femoral extension osteotomies are invasive procedures with significant associated risks 13. A recent retrospective study by Stout et al analysed the outcome in 73 children with crouch gait following distal femoral extension osteotomies with or without patella tendon advancement. The children in this study were divided into three groups; those who had a distal femoral extension osteotomy only, those who had a patella tendon advancement only and those that that had a combination of the two procedures. It was found that femoral extension osteotomy in conjunction with patella tendon advancement was necessary for achieving optimal results14. These results are unsurprising since the acute correction produced by an extension osteotomy of the femur almost always results in slackening of the extensor mechanism and this necessitates performing a secondary re-tensioning procedure to prevent an extensor lag postoperatively. The 8-plate technique through the process of gradual correction has a theoretical advantage in this respect. None of the patients in our series required a secondary procedure to re-tension the extensor mechanism. This was further substantiated by a lack of change in the Koshino Index with gradual correction of the knee flexion contracture.
Hamstring release is a popular procedure. Beals evaluated surgical factors influencing prognosis for ambulation and found that although surgery rarely changed the mode of ambulation, hamstring release was unique as 5 of the 7 non-ambulatory patients in his series treated by the above procedure became crutch walkers in one year7. Proximal hamstring release has become unpopular, as the incidence of iatrogenic genu recurvatum and increase in lumbar lordosis have been found to be unacceptably high15. Distal hamstring release is popular but this is associated with recurrence rates of between 35 and 40%5,11.
Haas et al showed in 1948 on experiments in dogs that wire loops or staples applied unilaterally across the growth plate causes arrest of growth on the side of insertion compared to the other side16. Femoral hemiepiphysiodesis using staples has been used for correction of frontal and sagittal plane deformities, since Blount et al popularised it to control growth at the epiphysis17. Staples typically cause a sudden arrest of growth. Complications such as migration of staples, fatigue failure and risk of physeal closure have decreased the popularity of this procedure in recent times18,19,20.
The ideal procedure should be easy to perform, reversible, extra periosteal and extra physeal. Stevens et al have effectively used it in correction of frontal plane deformities1 and more recently in the correction of fixed flexion contractures2. The above mentioned study reviewed a series of 18 patients (29 limbs). A mean correction of 15 degrees was achieved at a mean follow up of 14 months. Staples as mentioned above produce sudden correction. We have had one complication to date, failure of the distal screw at the screw head-to-shaft interface in a patient who failed to attend several follow-up appointments. This complication of the 8-plate has not been reported previously in the literature. The 8-plate device is designed to allow divergence of the screws to approximately 30 degrees. Due to a lack of regular follow-up, screw divergence continued beyond 30 degrees and failure occurred at 43 degrees of divergence. This case highlights the importance of regular clinical and radiographic follow-up until plate removal or physeal closure whichever occurs earlier. The shortcomings of this study are that it is retrospective and potential for variations in measuring flexion contractures of the knee using a handheld goniometer. Long term follow up is planned to determine if the promising early results meet long-term expectations. GMFCS level was not recorded as the intervention was not targeted at children with cerebral palsy but it may be that the ambulators benefitted to a greater extent than non-ambulatory children.
Based on our experience with using the 8-plate technique we would recommend the following to surgeons intending to use this technique for the correction of knee flexion contractures.
- Careful regular follow-up at 4 monthly intervals with lateral radiographs of the knee is required. Caution needs to be exerted in children from families who have demonstrated poor compliance with regular out-patient follow-up. The possibility of screw breakage during treatment or at the time of removal should be included in the list of possible complications.
- The rate of correction coincides with the rate of growth. It would therefore stand to reason to time the intervention with the period of maximal growth. In practice, this is rarely possible. This is of particular importance when the 8-plate technique is employed as part of SEMLS.
- In children with flexion contractures greater than 40 degrees, the technique should be employed in conjunction with pre-operative serial casting and/ or hamstring release. In our experience, the 8-plate technique is effective where the residual deformity is less than 40 degrees.
- In children where the plate has been implanted for longer than 18 months, the implant may be buried within the epi-metaphyseal region due to appositional growth. The risk is particularly greater in children under the age of 10 years. In our experience, there were no instances of permanent physeal arrest at latest follow-up. We have successfully revised buried plates with no apparent ill-effects to date.
Conclusion:
This study was performed to confirm whether temporary epiphysiodesis can reliably correct knee flexion contractures therefore we used anatomical outcome measures. Functional and gait laboratory data outcome measures were not used as patient group was too diverse and many other interventions were employed at the time of epiphysiodesis to make useful conclusions.
We believe that our data demonstrates that using the 8 plate can reliably correct knee flexion deformities under 40 degrees and is a simple technique to learn and perform with low complication rates.
Figures:

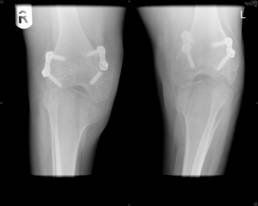
Figure 1: X ray showing divergence of screws
`
Figure 2: X-Ray showing broken screw
Reference :
- Stevens PM. Guided growth for angular correction. A preliminary series using a tension band plate. J Pediatr Orthop. 2007;27(3): 253-59.
- Klatt J, Stevens PM. Guided growth for fixed knee flexion deformity. J Pediatr Orthop. 2008; 28(6): 626-631.
- Koshino T, Sugimoto K. New measurement of patellar height in the knees of children using the epiphyseal line midpoint. J Pediatr Orthop. 1989;9:216-18
- Keats S, Kambin P. An evaluation of surgery for the correction of knee-flexion contracture in children with cerebral spastic paralsysis. J Bone Joint Surg Am.1962;44:1146-54
- Ma FYP, Selber P, Nattrass GR, Harvey AR, Wolfe R, Graham HK. Lengthening and transfer of hamstrings for a flexion deformity of the knee in children with bilateral cerebral palsy. J Bone Joint Surg.2006;88(2):248-54
- Beals RK. Treatment of knee contractures in cerebral palsy by hamstring lengthening, posterior capsculotomy and quadriceps mechanism shortening. Dev Med Child Neurol. 2001 Dec;43(12):802-5
- Beals RK. Spastic paraplegia and diplegia. An evaluation of non-surgical and surgical factors influencing the prognosis for ambulation. J Bone Joint Surg Am. 1966 Jul;48(5):827-46.
- Cravener EK. Device for overcoming non-bony flexion contractures of the knee. J Bone Joint Surg Am.1930;12:437-39
- Hughes RE, Rissner JC. The correction of knee-flexion deformity, after poliomyelitis, by wedging plasters. J Bone Joint Surg.1934;16:935-46
- Hart VL. Corrective cast for flexion-contracture deformity of the knee. J Bone Joint Surg.1934;16:970-71
- Dhawlikar SH, Root L, Mann RL.Distal lengthening of the hamstrings in patients who have cerebral palsy. Long-term retrospective analysis. J Bone Joint Surg Am. 1992 Oct;74(9):1385-91
- SL Haas. Correction of extreme flexion contracture of the knee joint. J Bone Joint Surg.1938;20:839-50
- Zimmerman MH, Smith CF, Oppenheim WL. Supracondylar femoral extension osteotomies in the treatment of fixed flexion deformity of the knee. Clin Orthop and Relat Res.1982;171:87-92
- Stout L J, Gage J R, Schwartz M H, Novacheck TF. Distal femoral extension osteotomy and patellar tendon advancement to treat persistent crouch gait in cerebral palsy. JBJS 2008 Nov; 90(11): 2470-84
- Drummond DS, Rogala E, Templeton J, Cruess R.Proximal Hamstring release for knee flexion and crouched posture in cerebral palsy. J Bone Joint Surg Am.1974;56:1598-1602
|

