|
Abstract:
Aseptic fibrosis, local necrosis, or loosening of a device secondary to metallic corrosion and release of wear debris, is a classical description of metallosis. We are presenting a severe case of Tantalum metallosis of a right total hip revision, which only lasted 2 years. Our patient developed classical symptoms and radiological findings of metallosis. The cause of the loosening was due to her acetabular implants, a Tantalum trabecular cup and restrictor, which had been rubbing on one another, thus producing a severe metallosis reaction. Her intra-capsular fluid was creamy-white and her histopathological findings differ from the classic description. Tantalum metallosis of such severity has not been described in the literature before, this is a rare example of metallosis and its much perplexing nature.
J.Orthopaedics 2012;9(3)e9
Key Words
Tantalum; metallosis; revision hip arthroplasty; restrictor;
Introduction:
Metallosis has been a recent topic in the literature that is being more pursuit by researchers and clinicians, as it affects more patients than thought of initially. It leads to early loosening of prosthesis and difficult revision surgery. The overall incidence of metallosis in revision total hip arthroplasties was found to be 5.3%. The most common signs of metallosis on radiographs are osteolyis (77.4%), metal particles (45.2%) and the bubble sign (32.3%)[
Chang JD, Lee SS. Revision Total Hip Arthroplasty in Hip Joints with Metallosis, J Arthroplasty. 2005 Aug;20(5):568-73.] [ E.P. Su, P.W. Callander and E.A. Salvati, The bubble sign: a new radiographic sign in total hip arthroplasty, J Arthroplasty 18 (2003):110]. The most common histopathological findings are perivascular lymphocytic infiltrate, histiocytic changes, metal particles visible under polarized light, foreign body giant cells, fibrin exudation and necrosis[ Michael A. den Bakker, Metallosis in revision knee arthroplasty, Internet Journal of Pathology 2005, Volume 4, Number 2].
The Mirra classification is used to determine the severity of the metallosis on a histopathological level[Doorn PF, Mirra JM, Campbell PA, Amstutz HC. Tissue reaction to metal on metal total hip prostheses. Clin Orthop Relat Res. 1996;(329 Suppl):S187-205.].
We are presenting a 69 year old patient who has developed a severe case of metallosis, of her right total hip replacement. She has under gone revision surgery two years ago with a Zimmer® Tantalum trabecular metal (TM) cup, a TM central restrictor and bone graft was performed 2 years earlier. Her original total hip replacement was peformed 14 years earlier.
She presented with pain over three months duration, which was getting worse.
She was unable to weight bear for the last three days before presenting to the hospital. She had an extensive medical and surgical background, the major things being hypertension, hypercholesterolemia, ischaemic heart disease, non-insulin dependant diabetes mellitus, gout, two clipped cerebral aneurisms, bilateral THR, cervical cancer, colostomy secondary to fistulae formation from radiotherapy.
Her initial examination did not reveal any signs of infections. Her range of movement was severely restricted by pain. She could not weight bear.
She denied any fevers, rigors, falls or trauma.
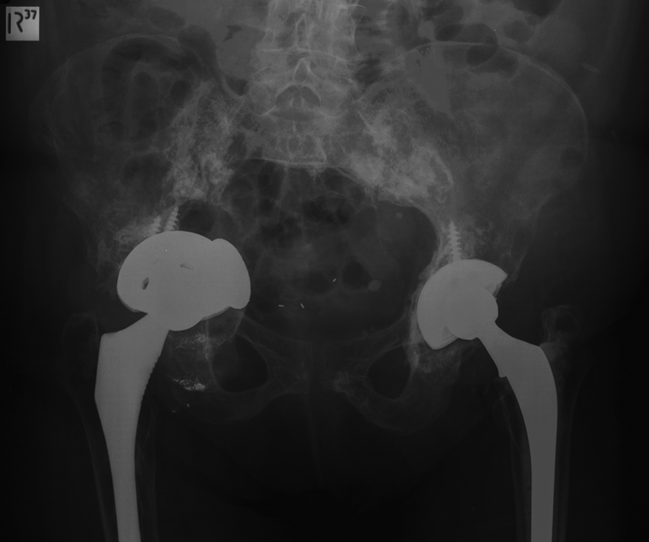
Her blood screen was unremarkable, with a white cells count of 9.6x109/L, platelets of 225x109/L, haemoglobin of 149g/L, a CRP of 5.6 and an ESR of 30. Her radiograph showed a classical metallosis picture of osteolysis around the acetabular component, with protrusion of the central TM restrictor into the pelvis, metal particles surrounding the hip and a bubble sign[
] (Fig 1).
Figure 1 Radiograph showing the protrusion of the Tantalum Cap and the Bubble sign.
A differential diagnosis of metastatic disease, aseptic loosening or septic loosening was followed, and she underwent an USG guided aspirate of her right hip, which was reported as frank pus by the radiologist. It was decided that she should be taken to theatre for a first stage revision surgery.
A modified Hardinge approach was used to gain access to the hip joint. The joint capsule was incised and large amounts of creamy/white glossy fluid escaped under pressure, which has been sent to microbiology. The joint capsule was hypertrophic and was sent for histopathology. Sever osteolysis with pelvic discontinuity was found loosening of the acetabular component and a medial acetabular wall defect. The femoral and acetabular components were removed, and excision arthroplasty was peformed.
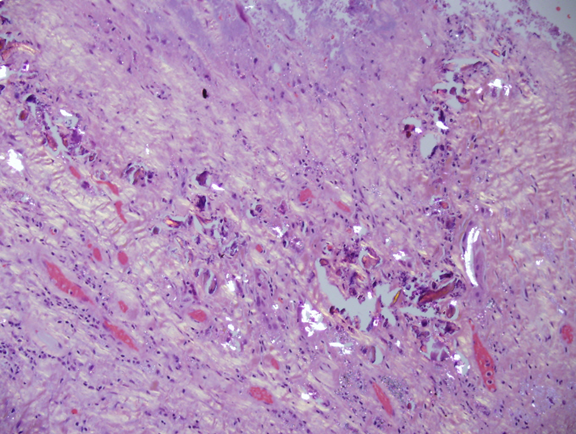
The cause of the loosening was presumed to have occurred due to her acetabular implants. The tantalum trabecular cup and the restrictor, which had been rubbing on one another, thus producing a severe metallosis reaction (Fig 2). The final microbiology results were negative for an infection from the initial USG guided aspirate as well as from the surgery itself. The histopathological changes were very unusual, as there was no perivascular infiltrates, there was an abundant amount of amorphous substance with small metal particles, much finer than the particles in the joint capsule and dystrophic calcifications (Fig 3).
Unfortunately, as the patient was investigated further, large masses in her lungs were found and biopsied, revealing primary adenocarcinoma of lung.
Figure 2 The retirved acatabular cup and the central restrictor.

Figure 3 – Histopathological slide with polarized light showing the metallosis.
Discussion:
A far as we are aware, there has not been a publication in the English literature on such a catastrophic failure due to Tantalum metallosis. We believe the failure of this revision was due to incorrect placement of the Tantalum Central Restrictor and inadequate bone grafting between the restrictor and the acetabular component. This gave the possibility of direct contact between the two implants, and extreme Tantalum debris formation.
Tantalum, Ta 73, is a grey-blue metal which has extremely high resistance to corrosion, its name comes from Greek mythology.[ The father of Niobe, who has been punished by the Gods, after death by being condemned for eternity to stand neck deep in water with ripe fruit growing above him. If he tried to drink the water, it drained below the level of his reach, and if he reached for the fruit, the branches moved upward, being out of his grasp.] It has been used in the production of electronic components, capacitors and resistors, jet engine components, nuclear reactors, and missile parts. In orthopaedics, it is used for implants, such as THR, due to its natural properties.
We believe that Tantalum has different properties on a cellular level, thus produces different microscopic and macroscopic changes. The histopathology that we have received back, clearly showed an absence in perivascular lymphocytic infiltrates, this might be due to the fact that Tantalum has low biological reaction. We cannot explain why the colour of the intra articular fluid was cream/white.
Our theory is this could be due to the natural properties of Tantalum. Whilst titanium stains black, cobalt-chrome stains greyish/green, from our experience we can report that Tantalum sains creamy/white. There are many positive properties of Tantalum, such as its strength and low inflammatory reaction to tissues, and as this new metal will be ever more used in arthroplasties and other surgical implants we have to research its properties more closely with large retrospective studies and observe its local and generalised reaction to tissues.
From this case repost we advise to use plenty of bone graft to interpose between the acetabulum component and the central restrictor, as well as between the central restrictor and the acetabular wall it self.
Reference:
Chang JD, Lee SS. Revision Total Hip Arthroplasty in Hip Joints with Metallosis, J Arthroplasty. 2005 Aug;20(5):568-73.
E.P. Su, P.W. Callander and E.A. Salvati, The bubble sign: a new radiographic sign in total hip arthroplasty, J Arthroplasty 18 (2003):110
Michael A. den Bakker, Metallosis in revision knee arthroplasty, Internet Journal of Pathology 2005, Volume 4, Number 2
Doorn PF, Mirra JM, Campbell PA, Amstutz HC. Tissue reaction to metal on metal total hip prostheses. Clin Orthop Relat Res. 1996;(329 Suppl):S187-205.
|

