|
Abstract:
Introduction: Osteointegration of uncemented acetabular component is essential for its long-term stability. To avoid the potential problems associated with screws that are often used to obtain their initial stability, oversizing of the component has been recommended. The objective of this study was to analyse the periacetabular gaps in the early post-operative period for osteointegration of hydroxyapatite-coated acetabular cups inserted with the press-fit technique.
Methods: 53 primary uncemented total hip arthoplasties performed at our hospital by a single surgeon between February 2003 and August 2005 were involved in this study. There were 29 females and 22 males. Mean age of patients was 70 years (range, 52-88 years). Periacetabular gaps were measured on the radiographs taken at day-1 post-operatively and at 3 months follow-up. All the measurements were taken independently by two investigators on two different occasions using a Picture Archiving & Communications (PACS) System. The two sets of data from each investigator were compared for intra and inter-observer variability using independent-samples t test.
Results: In 24 cases, no gaps were found around the acetabular cups on day-1 post-operative radiographs. In 29 cases, the mean gap was 4 mm (range, 1-8 mm) on post-operative day-1. Five gaps were in zone one, 24 in zone two and none in zone three. At 3 months follow-up, the mean gap was found to be 0.6 mm (range, 0-3 mm). The reduction in gaps from day-1 post-op to 3 months follow-up was statistically significant (Chi square test, p<0.05).
Discussion: We found a significant fill-in of periacetabular gaps as early as at 3 months suggesting osteointegration of hydroxyapatite-coated acetabular cups inserted with press-fit technique.
J.Orthopaedics 2012;9(3)e6
Keywords:
Total hip replacement; Uncemented acetabular cup; Periacetabular gap
Introduction:
In the early to mid-1980s, numerous types of surfaces and porous coatings were incorporated into press-fit acetabular cups to provide biological fixation to bone. Early radiographic findings for the first-generation uncemented acetabular cups showed a significant proportion without direct apposition to the implants in one or more acetabular interface zones. This, in large part, was attributed to the accepted surgical technique of the time, namely, line-to-line fit which led to a low incidence of zone II gaps, but a more frequent occurrence of gaps in zones I and/or III. Beginning in the early 1990s, most manufacturers introduced new designs and improved manufacturing techniques that increased the mechanical reliability of acetabular cups, which in turn increased the general biologic harmony between host bone and the cup. The surgical technique evolved to press fitting the acetabular cup which led to a lower prevalence of gaps in zon
es I and/or III, but an increased occurrence of gaps in zone II.
A good primary stability of an uncemented cup can be achieved by the press-fit technique, inserting an oversized cup into the underreamed acetabulum.1-3 Recommended differences of the diameter between the last used reamer and the finally used cup range from 1 to 3 mm.1,4,5 In this manner the cup is fixed at the outer diameter of the acetabulum, which leads to uniform transfer of load and homogeneous, approximately physiological loading of the acetabulum.5 Animal studies have shown the osteoconductive effects of HA coating even in loaded and initially unstable implants.6,7 In clinical use, promising short- to mid-term results with HA-coated hip implants have been reported.8,9
The current study examined the thickness and extent of periacetabular gaps that occurred when the technique of underreaming the acetabular surface (oversizing the acetabular component) was used to obtain the fixation. The objective of this study was to assess these gaps radiologically for the evidence of osteointegration at the metal-bone interface with HA-coated press-fit acetabular cups in the early post-operative period.
Methods
53 primary uncemented total hip arthoplasties were performed at our hospital by a single surgeon (APW) between February 2003 and August 2005. There were 29 females and 22 males. Two patients had bilateral surgeries. Mean age of patients was 70 years (range, 52-88 years). The underlying diagnosis was primary osteoarthritis of the hip in all the patients. All the procedures were performed by anterolateral approach to the hip in supine position. HA-coated acetabular cups (SecurFit, Stryker Howmedica Osteonics, NJ) and uncemented femoral stems (Omnifit-HA; Osteonics, Allendale, New Jersey) were implanted in all the cases. The cups had a fifty-micrometer-thick coating that consisted of more than 90% hydroxyapatite.
The coating had been plasma-sprayed onto the titanium substrate, which had been roughened previously by beadblasting to a surface finish of three to four micrometers. There were no screw holes or stabilizing spikes or pegs. The acetabular cups were inserted using a press-fit technique. The acetabulum was prepared with even-diameter reamers until all of the cartilage had been removed and healthy bleeding bone was exposed. A trial component of the same size as the last
reamer was then impacted into the acetabular component. The coverage and contact with the host bone was inspected, and the stability of the trial component was checked by wobbling the shell holder.
To achieve press fit stability, a prosthesis 2 mm larger than the trial component was used. Bone grafts were not used in any case. The stability of acetablar cups was found to be satisfactory by manual assessment intra-operatively.
All the patients were advised partial weight bearing with two crutches for six weeks post-operatively. Crutches were discontinued at six weeks and full weight bearing was allowed. Anteroposterior pelvic radiographs were obtained for all patients preoperatively, on day-1 postoperatively and at 3 months follow-up in the same department with the patient in a decubitus position and with a vertical beam centred on the pubic symphysis.
The distance between the source and the plate was one metre. Periacetabular gaps were measured on the radiographs taken at day-1 post-operatively and at 3 months follow-up. Gaps were defined as areas of apparent decreased density in which the surface of the acetabular component was not in contact with bone. Such gaps were recorded as present when it involved 50% or more of the zone in which it was situated. If a gap was identified, the width was measured to the nearest millimetre using a Picture Archiving & Communications (PACS) System. The acetabulum was divided in to three equal zones using DeLee and Charnley method.10 A component was considered to have migrated if change in position was greater than 3 mm and/or 80 with respect to the baseline film.
All the measurements were taken independently by two investigators on two different occasions. The observers were blinded from all patient- and implant-related demographics as well as the clinical status of each patient. The two sets of data from each investigator were compared for intra and inter-observer variability using independent-samples t test.
Results
In 24 cases, no gaps were found on day-1 post-operative radiographs. In 29 cases, the mean gap was 4 mm (range, 1-8 mm) on post-operative day-1. Five gaps were in zone I, 24 in zone II and none in zone III. The gaps were mostly situated in the polar region, that is zone II, when compared with the peripheral zones.
The distribution of the width of the initial gaps was as shown in table 1. No osteoarthritic cystic lesions were observed at the interface between the cup and bone. The gap interface analysis at 3 months follow-up showed that 22 out of 29 gaps (76%) were no longer radiologically evident. Of the remaining seven gaps, 2 were in zone I, 5 in zone II and none in zone III. All the gaps that initially were less than 1 to 3 mm in width (17 cases) had become undetectable upon 3 months follow-up. The mean gap at 3 months was found to be 0.6 mm (range, 0-3 mm). The distribution of the width of gaps at 3 months was as shown in table 2.
The reduction in gaps from post-operative day-1 to 3 months follow-up was statistically significant (Chi square test, p<0.05). There was no evidence of progression in width or extent of any of the initial gaps. None of our cups migrated radiologically.
Discussion
Various studies have reported a frequent occurrence of periacetabular gaps with uncemented cups in the early postoperative period.2,3,11,12,13 In a laboratory study using cadaveric acetabuli, Mackenzie et al found gaps to be less than 1mm for line-to-line fit, whereas 1.4 and 3.9 mm polar gaps were found for 2 and 4 mm press-fit cups.3 Onsten reported fill-in of 4 and 5 mm gaps during a follow-up period of 30 to 40 months for 2 patients with line-to-line surgical preparation and autologous morselized bone graft.11 Gruen et al, in a multicentre study, reported post-operative acetabular gaps mainly in zone II with press-fit cups in 80 (19%) of 414 hips.14 They reported that gaps of 4 to 5 mm closed within two years. Roth et al described zone II gaps in 18% cases with press-fit cups that disappeared within two years.15
Macheras er al showed a complete fill-in of gaps from 1 to 5 mm in width in 25 hips within six months of the operation with trabecular metal monoblock acetabular components.12
Physical interlocking between the cup and the supporting bone beneath it is a prerequisite for its long-term stability. Hydroxyapatite (HA) coating is known to cause osteointegration of the uncemented acetabular cups.6,7 Although augmentation screws enhance stability, potential concerns include fretting between the screws and metal acetabular components, inadvertent screw penetration into neurovascular structure and tracking of polyethylene debris along the path of the screws.16,17 Stable acetabular fixation using an underreaming technique without screw augmentation is an appealing alternative that would alleviate all of the concerns associated with screw fixation.2
Hermida et al reported a mean 32% reduction of radiolucent line length at 2 to5 years follow-up with hydroxyapatite-coated cups.13 We found a significant reduction in periacetabular gaps as early as at 3 months with HA-coated press-fit cups. There are no previous studies in the literature that have reported fill-in of gaps as early as at 3 months. Our study shows a reliable osteointegration of HA-coated cup inserted with a press-fit technique in the early post-operative period. We feel that screws fixation for these cups is not necessary due to an early osteointegration with the host bone as shown in this study.
References
Adler E, Stuchin SA, Kummer FJ. Stability of press-fit acetabular cups. Journal of Arthroplasty 1992; 7: 295301
.
Dorr LD, Wan Z, Cohen J. Hemispheric titanium porous coated acetabular component without screw fixation. Clinical Orthopaedics and Related Research 1998; 351: 158-168.
MacKenzie JR, Callaghan JJ, Pedersen DR, Brown TD. Areas of contact and extent of gaps with implantation of oversized acetabular components in total hip arthroplasty. Clinical Orthopaedics and Related Research 1994; 298: 127-136.
Curtis MJ, Jinnah RH, Wilson VD, Hungerford DS. The initial stability of uncemented acetabular components. Journal of Bone and Joint Surgery British Volume 1992; 74: 372376.
Morscher E, Masar Z. Development and first experience with an uncemented press-fit cup. Clinical Orthopaedics and Related Research 1988; 232: 96103.
Soballe K, Hansen ES, Brockstedt-Rasmussen H, Bunger C. Tissue ingrowth into titanium and hydroxyapatite coated implants during stable and unstable mechanical conditions. Journal of Orthopaedic Research 1992; 10: 285-299.
Tisdel CL, Goldberg VM, Parr JA, Bensusan JS, Staikoff LS, Stevenson S. The influence of a hydroxyapatite and tricalcium-phosphate coating on bone growth into titanium fiber-metal implants. Journal of Bone and Joint Surgery American Volume 1994; 76-A: 159-171.
Geesink RGT. Hydroxyapatite-coated total hip prostheses. Two-year clinical and roentgenographic results of 100 cases. Clinical Orthopaedics and Related Research 1990; 261: 39-58.
Kroon PO, Freeman MAR. Hydroxyapatite coating on hip prostheses: effect on migration into the femur. Journal of Bone and Joint Surgery British Volume 1992; 74-B: 518-522.
DeLee JG, Charnley J. Radiographic demarcation of cemented sockets in total hip replacement. Clinical Orthopaedics and Related Research 1976; 121: 20-32.
Onsten I, Carlsson AS, Sanzen L, Besjakov J. Appositional bone bridging of primary gaps in the dome area of uncemented, porous acetabular components. Journal of Arthroplasty, 1995; 10: 702-706.
Macheras GA, Papagelopoulos PJ, Kateros K, Kostakos AT, Baltas D, Karachalios TS. Radiological evaluation of the metal-bone interface of a porous tantalum monoblock acetabular component. Journal of Bone and Joint Surgery British Volume 2006; 88-B: 304-309.
Hermida JC, DLima DD, Steklov N, Colwell CW Jr. Outcome of an acetabular design with hydroxyapatite coating on a rough substrate. Clinical Orthopaedics and Related Research 2005; 441: 298-304.
Gruen TA, Poggie RA, Lewallen DG, Hanssen AD, Lewis RJ, OKeefe TJ et al. Radiographic evaluation of a monoblock acetabular component. Journal of Arthroplasty 2005; 20: 369-378.
Roth
A, Winzer T, Sander K, Anders JO, Venbrocks RA. Press fit fixation of cementless cups: how much stability do we need indeed? Archives of Orthopaedic and Trauma Surgery 2006; 126: 7781
Ng FY, Zhu Y, Chiu KY. Cementless acetabular component inserted without screws-the effect of immediate weight-bearing. International Orthopaedics 2007; 31: 293-296.
Keating E, Ritter M, Faris P. Structures at risk from medially placed acetabular screws.
Journal of Bone and Joint Surgery American Volume 1990; 72A: 509-511.
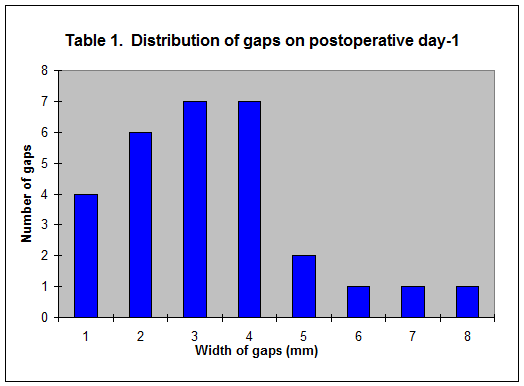
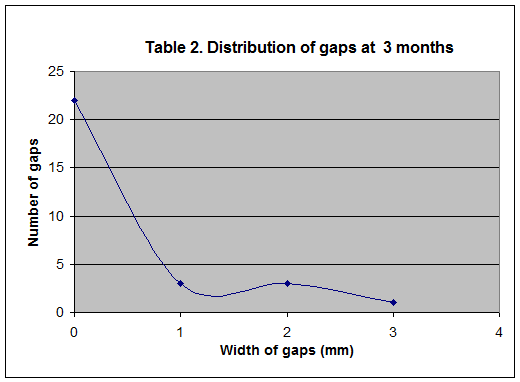
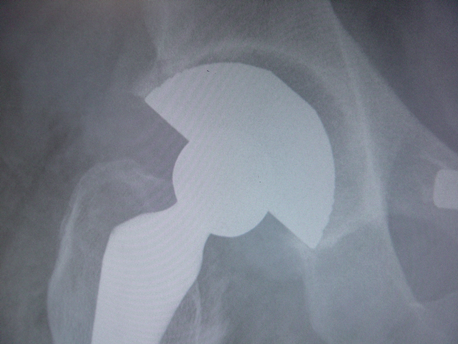
Figure 1 (A): Case one: 6 mm gap in Zone II on postoperative day-1
radiograph in a 67 year old man

Figure 1 (B): Case one: Complete fill-in of gap at three months follow-up

Figure 2 (A): Case two: 3 mm gap in Zone II on postoperative day-1
radiograph in a 62 year old man

Figure 2 (B): Case two: Complete fill-in of gap at three months follow-up
|

