|
Abstract:
Purpose: For arthroscopic suture in rotator cuff tear, there are many various surgical methods being introduced recently so as in many cases it is difficult to determine which type of method is ideal for Rotator Cuff Repair. To this end, we intended to introduce and compare procedural techniques of Ulsan University Suture (UU Suture -8 Anchoring Suture) with those of the Mason-Allen suture commonly known to be the most powerful.
Procedural Techniques: UU Suture is a stitching technique of using banana-shape stitching needle by passing it the anterior side of rotator cuff via the anterior portal approach followed by passing it through the posterior side and PDS, placing it at the anterosuperior portal and create a shuttle-relay to PDS, then hook the suture between them, pull and pass it through the rotator cuff. Using the same method, pass the suture by using a banana-shape stitching needle by posterior portal approach from the posterior side of rotator cuff toward the anterior and by placing it at anterosuperior portal, the preparation for UU Suturing can be completed. MA Suture uses a method with a suturing hook at the anterior portal by procedures to stitch the posterior side for about 0.5~1cm of the end margin of rotator cuff tear and passes the suture through PDS, creates shuttle-relay and let the suture pass it. Using the same method, let the suture pass by using a suturing hook in posterior portal approach and stitch the slightly anterior side of rotator cuff tear margin. Then, MA Suture method is completed by pulling both ends of suture from the anterosuperior portal. Both procedural techniques can anchor the suture using interference screws.
Conclusion: If anyone feels the MA Suture is difficult to perform, it is considered that the use of UU Suture can be recommended. UU Suture is a simple but excellent method usable for arthroscopic rotator cuff repair and as an alternative method analogue and equivalent to Mason-Allen Suture in arthroscopic rotator cuff repair .
Keywords:
UU suture, MA suture, Rotator cuff, Arthroscopic repair
J.Orthopaedics 2012;9(3)e10
introduction
Currently, the frequency of rotator cuff injuries is increasing according to the increase of the elderly population as well as the increase of sports activities as a trend, and owing to the advancement of arthroscopy and diagnostic techniques, diagnosis and treatment of such injuries got much easier. Also increase of interest in rotator cuff diseases and advancement of medical technology had contributed to continual development and fast growth of unique and original methods to repair rotator cuff tear. However, as too diversified surgical methods are being introduced before any verification of such surgical m
ethods through analysis of clinical outcomes, so there are many cases that are difficult to determine which kind of surgical procedure would be ideal for rotator cuff repair. The ideal suturing method for rotator cuff repair should be the one that can minimize tendon-bone gap formation at the repair site with high level of torque strength and can manifest mechanical strength durable for repetitive loads so ultimately it should be able to obtain biological healing of tendon-bone tissues. The authors introduce UU Suture and compared it with MA Suture commonly known to be the most powerful.
Procedural Techniques
- Preparation and Creation of Insertion Portal
The surgery was performed in patient lying at 70 degree sitting posture (beach-chair position) under general anesthesia. The diagnostic arthroscope was advanced into shoulder joint and performed the arthroscopy on the scapulohumeral joint and thereafter it was possible to identify the ruptured rotator cuff with the arthroscope inserted into subacromial space. First, the thickened bursa was partially removed using motorized shaver and electrocauterized device by the anterior portal approach. Then a spinal needle was inserted from the inferior side at about 1 inch away from the acromion margin into the site where the rotator cuff tear had incurred and it had enabled identification of the center region of tear from the above of skin.
An external entrance portal was formed at where the spinal needle had entered and performed subacromial decompression by inserting electrocauterized device and motorized shaver alternatively.
The position of tear was confirmed by advancing the spinal needle into the subacromial space from the skin in the middle portion of the external and the posterior portals, and a 2 ~ 3 mm skin incision was at the location identified and made the posterolateral portal.
Through the portal, the rotator cuff tear was identified, the coronoid process was found and the operability was improved by subcoracoid release and dissecting the adhesion at infrascapular spine
- UU Suture-utilized arthroscopic procedure techniques
A banana-shape stitching needle was inserted into the anterior portal, and lifted the anterior part of rotator cuff tear in use of retriever inserted into the anterosuperior portal so that the banana-shape stitching needle could pass through and subsequently lifted the posterior part of rotator cuff tear with retriever, allowed the banana-shape stitching needle to pass simultaneously. Then penetrated No. 1 Polydioxanone suture (PDS; Ethicon, Somerville, NJ) through the space between the needles and grabbed PDS only with grasper located at the anterosuperior portal and pulled the banana-shape stitching needle out first from the posterior subscapular infraspinous site.
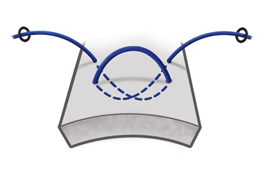
A shuttle-relay was made outside of the joint to PDS and the suture (Fiberwire, Arthrex. Naple. FL) was hooked to the gap and pulled so that it could pass through the rotator cuff, and the one end of passed suture was pulled out through the anterosuperior portal (Fig. 1). Using the same method, the suture was passed through the rotator cuff using the banana-shape stitching needle from the posterior portal and PDS was pulled out using the grasper located at the anterosuperior portal. Also a shuttle-relay was made to the PDS exited to the extra-articular lateral side of anterosuperior portal (Fig. 2) and hooked the previously pulled out suture then pulled it tight so that a U-shape loop was made at internal side of rotator cuff (Fig. 3).
By pulling both ends of suture from the anterior and the posterior sides through the anterosuperior portal, the preparation to perform UU Suture can be completed. And UU Suture can be completed by connecting 4.5 mm interference screws (Push-lock screw. Arthrex. Naple. FL) to both ends of suture and anchoring them to two humeral glenoid margins (Fig. 4).
- Mason-Allen Suture arthroscopic procedure techniques
The technique is to insert the suture hook (Suture Lasso, Arthrex, Naple, FL) into the anterior portal and make about 0.5~1 cm long stitch centering the tear end at 1~1.5 cm inner from the end margin of rotator cuff tear subsequent with passing PDS through. Then the PDS is pulled out using a grasper through the anterosuperior portal. Make a shuttle-relay to the pulled out PDS and connect the powerful suture (Fiberwire or Tigerwire, Arthrex, Naple, FL) to the connecting hook and let it pass through the rotator cuff in reverse direction. Afterwards, insert the suture hook into the posterior portal and make stitches to slightly forward from the end of rotator cuff tear and again let PDS pass through, then pull the PDS through the anterosuperior portal (Fig. 5).
Make a connecting hook to the PDS just pulled out, connect a previously pulled out strong suture to it, and pull it to reverse direction out then a horizontal mattress loop is formed as the suture passes through the anterior of rotator cuff. When pulling both ends of the strong suture (Fiberwire) out through the anterosuperior portal, the MA Suture is completed (Fig. 6). As two vertical hooks are hanging on the horizontal mattress, the horizontal mattress hook plays a role of checkrein to prevent the sutured rotator cuff tissues from re-tearing. The suture can be anchored using the interference screw at about 0.5cm lateral to the end of rotator cuff tear.
Discussion:
Recently, arthroscopic repair for a rotator cuff tear has been performed. Arthroscopic repair has been reported with several advantages 1-3). However, the arthroscopic repair takes a long time for familiarization as shortcomings, and the modified Mason-Allen suture closure could not be enforced, so it has known to have the intensity of suture as falling. The early re-tearing after arthroscopic repair, the suture causes premature failure of the cuff integrity (knot failure) or failure of suture (suture anchor failure) can be caused by the knot failure or the suture anchor failure, but the cause of most failures is said to be the pull out of suture through the rotator cuff. 4-5) Weak initial fixation and extension of suture form the distraction gap between the tendon-bone sealing and consequently sloppy tendon-bone healing will occur eventually.
Gerber et al argued that the anatomical state of rotator cuff repair is the most important prognostic factor than the size of the ruptured rotator cuff at the time of performing the repair.6)
MA arthroscopic suture (Arthroscopic Mason-Allen suture) had allegedly used two knots located to a vertical position through the same anchor, which was similar to a modified form of MA Suture 7). Such concept of arthroscopic MA suture repair is interesting, but its biomechanical natures still remain as unknown 8). It was claimed that when compared UU suture as a biomechanical experiment with the modified MA closure, both repair methods have similarities in terms of resistance to cycling loading and ultimate tensile load that causes the rupture 9).
We targeted the rotator cuff full thickness tear and performed the rotator cuff repair using arthroscopic UU suture then obtained good results from follow-ups over 1 year. In addition, when performed UU closure and modified MA (Mason-Allen) suture commonly known to be the most powerful using the most powerful material currently available, the biomechanical strength between UU suture and the modified MA suture had no significant difference 10)
Conclusion:
The authors consider that if performing MA suture is difficult technically, it is recommendable to use UU suture. UU suture can be a simple but excellent method usable for the arthroscopic rotator cuff repair, and it is considered as a similar alternative equivalent to Mason-Allen suture for the arthroscopic rotator cuff repair.
Reference:
1. Ellman H. Arthroscopic subacromial decompression analysis of one- to three-year results. Arthroscopy. 1987;3:173-81.
2. Gartsman GM. Arthroscopic treatment of rotator cuff disease. J Shoulder Elbow Surg. 1995;4:228-41.
3. Galatz LM, Ball CM, Teefey SA, Middleton WD, Yamaguchi K. The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears. J Bone Joint Surg Am. 2004;86:219-24.
4. Gerber C, Schneeberger AG, Perren SM, Nyffeler RW. Experimental rotator cuff repair. A preliminary study. J Bone Joint Surg Am. 1999;81:1281-90.
5. Ma CB, MacGillivray JD, Clabeaux J, Lee S, Otis JC. Biomechanical evaluation of arthroscopic rotator cuff stitches. J Bone Joint Surg Am. 2004;86:1211-16.
6. Gerber C. Massive rotator cuff tears. In :lannotti JP, Williams GR (eds): Disorders of the shoulder. Diagnosis and management. 1st ed, Philadelphia, Lippincott Williams & Wilkins Inc; 1999. 57-92.
7. Scheibel MT, Habermeyer P: A modified Mason-Allen technique for rotator cuff repair using suture anchors. Arthroscopy, 19: 330-333, 2003.
8. Ma CB, Comerford L, Wilson J, Puttlitz CM: Biomechanical evaluation of arthroscopic rotator cuff repairs: double-row compared with single-row fixation. J Bone Joint Surg Am, 88: 403-410, 2006.
9. Ko SH, Park KB, Jun HM, Kim TW, Lim HW, Yum YJ: Is the UU Stitch Really Alternative to Modified MA (Mason-Allen)
Stitch for Rotator Cuff Repair: Biomechanical Comparative Study of UU to Modified MA Stitch. J. of Korean Shoulder and Elbow Society, 12: 207-214, 2009.
10. Darren J, Ko SH, Park KB, et al. Is the UU Stitch Really Alternative to Modified MA (Mason-Allen) Stitch for Rotator Cuff Repair, -Biomechanical Comparative Study of UU to Modified MA Stitch. J Korean Shoulder Elbow Soc. 2009;12:207-14.
Fig. 1.
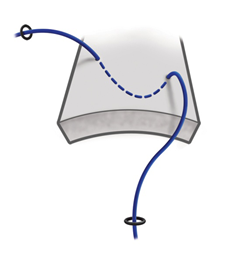
Fig. 2.
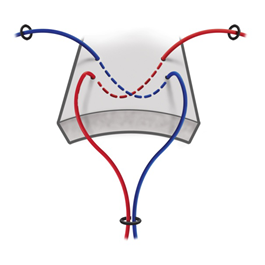
Fig. 3.

Fig. 4.
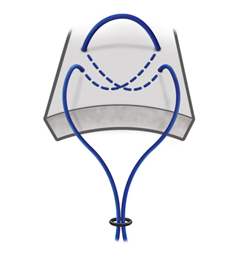
Fig. 5.
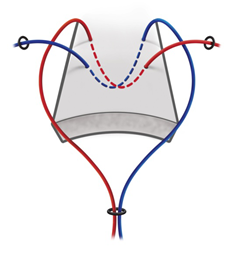
Fig. 6.
|

