|
Abstract:
Introduction: Purpose:
A systematic review published in 2006 found moderate evidence that intramedullary nailing lead to fewer complications than external fixation for paediatric femoral fractures but concluded that further research was necessary. We therefore aimed to review the literature published since and thereby update our understanding of which method has the lower complication rate.
Methods:
The Medline database (2005-present) was searched for studies comparing intramedullary nailing and external fixation that reported complications, defined as a residual deformity or an adverse event requiring secondary admission or surgery.
Results:
Five studies met the inclusion criteria, all Level of Evidence III. All the studies reported a higher complication rate with external fixation.
Conclusion:
This review provides further evidence that external fixation is associated with a higher complication rate than intramedullary nailing. However, the included studies have important methodological weaknesses. A well-designed prospective randomised trial is needed to compare the two methods.
J.Orthopaedics 2012;9(1)e10
Introduction:
The incidence of femoral fractures in children is 20 per 100,000 in the United States and Europe and they comprise 1.6% of all paediatric fractures 1-3. There is a bimodal age distribution, with peak incidences at two years and 12 years and they represent the most common major musculoskeletal injury in adolescents 4,5.
The aim of treatment is to provide suitable stability to allow fracture union with adequate alignment such that long term function is not compromised. It is generally thought that malalignment up to 30° in the sagittal plane and 10° in the coronal plane is acceptable, with no more than 10° of rotation or 2cm of shortening, depending on age 6.
Treatment was traditionally by skin or skeletal traction 7,8, with operative treatment reserved for open fractures or multiply-injured patients 9. Non-operative treatment however involves prolonged inpatient immobilisation and high costs 10. Attention has therefore turned to treatment modalities that facilitate early discharge from hospital, speeding return to activity while reducing the financial burden and the impact on patients and carers 11-13. Children up to the age of six can be treated with early hip spica 14,15, while the options for older children include plate osteosynthesis 16, external fixation 17,18, and rigid or flexible intramedullary nailing 19,20. The ideal technique should also preserve fracture biology, while minimising scarring and complications.
Plate osteosynthesis produces good results but requires much soft tissue dissection and subsequent
plate removal 21. Rigid intramedullary nailing may be useful in heavier children but risks avascular necrosis of the femoral head 22,23. External fixation has the benefits of minimal dissection, early weight-bearing and the ability to alter alignment and rigidity of the construct during treatment 24. It may however be complicated by pin site infections and re-fracture 25. Flexible intramedullary nailing is an effective treatment option but requires a skilled technician and is associated with residual deformity 26,27.
Poolman et al. performed a systematic review of the management of paediatric femoral fractures in 2006 28. They found moderate evidence that flexible intramedullary nailing reduced malunions and total adverse events compared with external fixation but concluded that further research was required. Our aim was therefore to review the literature published since this review was performed and, in doing so, to establish if external fixation (EF) or flexible intramedullary nailing (FIN) leads to fewer complications when treating femoral fractures in children.
Methodology:
A literature search was performed using the OvidSP interface to interrogate the Medline database on 8th December 2011. The search strategy is detailed in Table 1. Studies were included if they met the following criteria:
English Language
Original study
Comparative study (retrospective or prospective)
Study population with mean age <18 years
Fracture of the femur treated surgically
Data extractable about complications in a patient group treated with external fixation and a group treated with flexible intramedullary nailing
The most recent paper included in the systematic review by Poolman et al. was published in 2005. In order to update our understanding of this issue, only studies published since this year were included and work featured in the previous review was excluded.
Any study with a potentially relevant abstract underwent full-text assessment. Any disagreement regarding inclusion was resolved by consensus with the third author. Data was extracted by one author and verified by a second.
For the purposes of this review, a complication was defined as a residual malunion or leg length discrepancy (LLD), or an adverse event requiring hospital admission or another surgical procedure, other than planned removal of metalwork.
Table 1
1 |
External Fixators/ |
4398 |
2 |
external fixat*.mp. |
7539 |
3 |
Adolescent/ or Child/ or Child, Preschool/ or Infant/ |
2381629 |
4 |
paediatric.mp. |
26784 |
5 |
pediatric.mp. |
141878 |
6 |
child*.mp. |
1692906 |
7 |
Femoral Fractures/ |
11862 |
8 |
femur fracture.mp. |
747 |
9 |
femoral fracture.mp. |
1334 |
10 |
1 or 2 |
7539 |
11 |
3 or 4 or 5 or 6 |
2576784 |
12 |
7 or 8 or 9 |
12631 |
13 |
10 and 11 and 12 |
305 |
14 |
limit 13 to (english language and humans and yr="2005 -Current") |
|
Results:
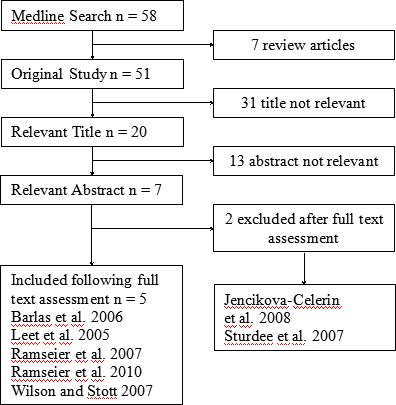
Five studies met the inclusion criteria. The process by which the studies included for critical appraisal were selected is explained in Figure 1. Following full text assessment, one study was excluded because results specific to those patients treated with external fixation could not be isolated from the reported data and one was excluded because the reporting of complications did not differentiate between treatment modalities 29,30.
Figure 1
The results of the five studies that met the inclusion criteria are summarised in Table 2. There is a trend towards increased complications in patients treated with external fixation compared to flexible elastic nails, particularly in terms of re-operations. The heterogeneity caused by differing definitions of complications and the lack of randomised controlled trials made pooled statistical analysis impractical. A narrative synthesis of the studies therefore follows, with mention of their key methodological weaknesses.
Table 2
Study |
EF Group |
FIN Group |
Other Findings |
Barlas & Beg 31 |
20 fractures
4 malunions
2 LLD
3 re-admissions |
20 fractures
No complications |
EF shorter operative time, more pain, more hip and knee stiffness
FIN shorter inpatient stay, higher parental satisfaction, quicker weight-bearing and return to school |
Leet et al. 36 |
59 fractures
15% complication rate |
45 fractures
13% complication rate |
Significantly higher complication rate and operative time in obese children
Shorter operative time in EF |
Ramseier
et al. 37 |
23 open fractures
91% complication rate |
12 open fractures
25% complication rate* |
Excluding pin track infections, EF group were 2.7 times more likely to have a complication
Shorter hospital stay in EF |
Ramseier
et al. 38 |
33 fractures in adolescents
48% re-operation
30% loss of reduction
9% malunion
6% LLD |
105 fractures in adolescents
8% re-operation
2% loss of reduction
7% malunion
1% LLD |
EF longer time to union and inpatient stay
EF group were 6.4 times more likely to have a major complication**
|
Wilson & Stott 39 |
21 fractures
3 re-operations
5 re-admissions
1 malunion |
20 fractures
3 re-operations
4 re-admissions
1 malunion |
EF group had longer hospital stay |
*unclear if complications occurred in rigid or flexible nails
** defined as a clinically relevant loss of reduction, a malunion or shortening, and/or a reoperation for any reason,
other than routine hardware removal
Barlas & Beg performed a small retrospective study of 40 children (average age 8.7 years) treated at one centre for femoral fracture over a four year period 31. It is not stated as to whether the centre has a specialised paediatric service. They report complications in 45% of patients treated with EF, compared to none in those receiving FIN. The EF group (n = 20) had shorter operative time but more post-operative pain and worse hip and knee range of movement. FIN group (n = 20) had shorter inpatient stay, higher parental satisfaction and quicker weight-bearing and return to school.
It is not clear if the 40 patients included in the study were consecutive patients, meaning there is a potential for selection bias. It seems unlikely that all the femoral fractures treated over the study period received EF or IMN but no data is provided about any fractures managed with other methods. Treatment allocation is unclear. They exclude Grade III open fractures and very proximal and distal fractures. Information is given on the total number of open fractures, associated injuries and fracture types but their spread between the two groups is not explained.
Although there is some explanation of operative technique, the level and experience of surgeon is not detailed, affecting reproducibility and applicability. There is also inconsistency among the FIN group, in which eight patients received stainless steel nails and 12 received titanium nails. These have been shown to result in different union rates and have different biomechanical properties 32,33,34.
The post-operative protocol differed between groups. The EF group were allowed to fully weight-bear while the the FIN were non- or partial weight-bearing. The basis of the decision to remove the fixation device is not stated. This is important information because re-fracture is a well-recognised complication of external fixation in these injuries.There is no information regarding the follow-up protocol.
The outcome measures in this study may not be relevant, in terms of malunion. The authors report sagittal or coronal malalignment of 5-10° in four patients in the EF group, and up to 1cm of LLD in two. These deformities are unlikely to be clinically significant and are within the generally accepted limits for paediatric femoral fractures. The reporting of other complications is limited to a table and whether these led to re-admission or repeat surgery had to be speculated for the purposes of this review. The reporting of complications did not meet the standards for outcome reporting in orthopaedic literature set by Papadokostakis et al. 35.
Although the main conclusion that FIN is a safe and effective technique is reasonable, they also conclude that external fixation should be used for highly comminuted fractures, although no analysis was performed regarding fracture type. In general, the methodological weaknesses and smll sample size of this study mean that its conclusions should be considered warily, although they are suitably understated.
Leet et al. performed a retrospective comparative to establish if obesity leads to more complications and longer operative times in surgical fixation of paediatric femoral fractures 36. They reviewed the surgical treatment of 104 femoral fractures in children with an average age of 9.3 years, finding a slghtly higher complication rate in those treated with external fixation.
There is no information regarding operative technique or which fixators or nails were used, reducing the reproducibility and applicability of the results. We are told that five paediatric orthopaedic surgeons treated the patients and treatment allocation was based on surgeon preference, introducing a potential selection bias.
Although we are told the overall complication rate for each treatment method, it is unclear which type of complication occurred with which method. This is not a failure of the study as it was not its primary purpose. That said, the conclusion drawn that obese children have a statistically significantly higher complication rate is possibly overstated given that only six of the 103 patients were obese. This study is unable to contribute significantly towards answering the question of this review.
The retrospective comparative study by Ramseier et al. investigated complications following external fixation and intramedullary nailing for open paediatric femoral fractures 37. Although these are rare injuries, it is a relevant and important topic as open fractures would often be accepted as an indication for external fixation. The rarity of the injury is highlighted by the fact that only 45 cases were identified over the 17 year study period at a major paediatric trauma centre. 23 were treated with EF, six with FIN, six with rigid nails and 10 by other means. They found that even after pin track infections were excluded, those treated with EF were 2.7 times more likely to have a significant complication.
The method of fixation was decided by the treating surgeon, representing an important source of selection bias. This may be reflected in the fact that 41% of the FIN group were Gustillo-Anderson Grade I, compared to only 17% of the EF group. The EF group tended to have more comminuted fractures. Flexible nails were introduced to the centre during the study period. It would be pertinent to know how many external fixators were used after their introduction.
The authors conclude that intramedullary devices should be used whenever possible in open paediatric femoral fractures, particularly in Grade I injuries. However, de
ep infection, possibly the most important complication of open fracture, was twice as common with nails. Although no reference is made to this specifically, they do suggest that initial external fixation prior to conversion to nailing may reduce deep infections.
While this paper is hindered by many of the short-comings of retrospective studies described previously, it is of value due to the comparatively large number of a rare injury. Furthermore, open fractures are often regarded as an indication for external fixation but this study seems to contradict this.
Ramseier et al. also performed a retrospective comparative study investigating four fixation methods in femoral fractures in adolescents 38. They found a significantly higher complication rate with EF, mostly loss of reduction requiring re-operation. Overall, those treated with EF were over six times more likely to suffer a complication than those treated with FIN. The study comes from a major centre specialising in paediatric trauma. One inclusion criterion was that patients should have been followed up until they regained their normal function. This potentially means that patients with the most severe complications causing prolonged loss of function may have been excluded from the study. Post-operative protocols regarding weight-bearing are not explained and there were inconsistencies regarding removal of metalwork.
There is no information about operative technique, the specific hardware used, or the experience level of the surgeon, reducing reproducibility. The method of fixation was decided by the treating surgeon and there are important differences between the groups that may highlight this. The EF group had more open fractures and more comminuted fractures than the FIN group.
The authors make conservative conclusions that seem to be reasonable, stating that FIN is an appropriate treatment method in heavier children and adolescents. They recognise that they may not be suitable for all fracture types. This is an important observation, given that more comminuted fractures in this study tended to be allocated to different fixation methods. While this study is imperfect due to its retrospective nature, it is a thorough and detailed assessment of a large number of patients which provides important information.
Wilson et al. aimed to establish what factors were associated with re-operations or re-admission following paediatric femoral fracture 39. Their retrospective review concluded that associated injuries cause prolonged inpatient stay, although time to initial operation was not a factor. Age was relevant, but this appeared to be due to the mechanism of injury and reflected the recognised bimodal distribution of femoral fractures. Children under six were generally admitted with low energy injuries, treated with an early hip spica and discharged soon after. Older children tended to suffer high energy fractures (for example road accidents) and have associated injuries, requiring surgical intervention. They had longer stays and higher re-admission rates, due to both the associated injuries and the complications of the surgical treatments. While not the primary aim of this study, the detailed reporting of the data allows us to extrapolate information relevant to complications. The EF group had a marginally higher complication rate than the FIN group.
The EF group were younger and more likely to have associated injuries than the FIN group (method of treatment allocation was not explained). There was no explanation of post-operative or follow-up protocols. There is no information about the hardware used or the experience of the surgeon. The reporting of complications is detailed but falls short of detailing fracture type and if the injury was open or closed.
Discussion:
These studies show a trend towards a higher rate of complications with external fixation compared to flexible intramedullary nails. That said, Leet et al. 36 and Wilson & Stott 39 failed to show a notable difference in complication rates but this was not the primary aim of these studies. Barlas & Beg had no complications in the FIN group but the study had some important methodological weaknesses 31. It should be noted that the two studies that report the greatest difference in re-operation rates were conducted at the same centre 37,38. Neither paper includes adequate information about treatment protocols. It may be that loose or infected external fixator pins that may have been removed in the clinic as part of routine follow-up in other centres were removed under general anaesthetic in this centre. For this reason, the results of these studies must be viewed with hesitance. Overall, the studies were similar in terms of age groups, fracture types and inclusion of open fractures (recognising that the two studies by Ramseier et al. were explicit in these areas). The outcome measures were similar between the studies, with consistency in the definition of a complication (if not in the definition of malunion). It should be remembered that any re-operation was often classified as a complication. One of the advantages of external fixation is that it allows alterations in alignment and rigidity during treatment. Procedures to alter the alignment of the fracture may have therefore been classified as a complication when actually they are an advantage.
Having found more complications with external fixation, it is not uncommon for authors to conclude that EF may still have a role in open fractures. It is therefore interesting to note that Ramseier et al. 37 found more complications after open fractures were treated with EF. It should be noted however that the EF group in this study contained more Grade II and III injuries.
Many of the complications in the FIN group may have been due to poor technique causing simple problems like prominent wires. The study periods of these studies often included the introduction of this technique to the centre and so included the learning curve of the new treatment which may have influenced the outcome. It may be that FIN proves to be clearly superior as surgeons become more experienced with this method.
As these studies show a higher complication rate with external fixation, even in open fractures, it seems that the indications for their use are diminishing. Polytrauma may remain an indication but surgeons may find that FIN can be performed as quickly as EF, as experience increases. Barlas & Beg 31 found that their last five nailings (once they had gained experience) took the same time as their average external fixator. Highly comminuted fractures may still require EF but biomechanical analysis has shown flexible nails to have equivalent stiffness when used in transverse and comminuted fractures 40. Complication rate is not the only consideration. These studies also found shorter inpatient stay and quicker union and return to activity with flexible nails.
The conclusions that can be drawn from these studies are limited due to the methodological weaknesses that have been highlighted. They can still be of use in generating a hypothesis for further investigation, forming the basis of a randomised trial. Poolman et al. 28 identified one randomised controlled trial comparing EF and FIN for paediatric femoral fractures 41. This was a small trial of only 20 fractures and there were questionable recruitment and randomisation protocols. Given the lack of clear benefits of EF, it may be difficult to approach this question from a position of equipoise, making a randomised controlled trial impossible. The area in which EF is likely to still have a role is the most severe cases but recruiting these cases into a randomised trial would be difficult.
Conclusions:
This review provides further evidence that external fixation is associated with a higher complication rate than intramedullary nailing, although the included studies have important methodological weaknesses. A well-designed prospective randomised trial is needed to compare the two methods.
Reference:
1. Rewers A, Hedegaard H, Lezotte D, Meng K, Battan FK, Emery K, et al. Childhood femur fractures, associated injuries, and sociodemographic risk factors: a population-based study. Pediatrics 2005;115(5):543-52.
2. Nafei A, Teichert G, Mikkelsen SS, Hvid I. Femoral shaft fractures in children: an epidemiological study in a Danish urban population, 1977-86. Journal of Pediatric Orthopedics 1992;12(4):499-502.
3. Bridgman S, Wilson R. Epidemiology of femoral fractures in children in the West Midlands region of England 1991 to 2001. Journal of Bone & Joint Surgery - British Volume 2004;86(8):1152-7.
4. Landin LA. Epidemiology of children's fractures. Journal of Pediatric Orthopaedics, Part B 1997;6(2):79-83.
5. Hinton RY, Lincoln A, Crockett MM, Sponseller P, Smith G. Fractures of the femoral shaft in children. Incidence, mechanisms, and sociodemographic risk factors. Journal of Bone & Joint Surgery - American Volume 1999;81(4):500-9.
6. Koval K. Handbook of Fractures, Third Edition. Philadelphia: Lippincott Williams & Wilkins; 2006.
7. Canale ST, Tolo VT. Fractures of the femur in children. Instructional Course Lectures 1995;44:255-73.
8. Levy J, Ward WT. Pediatric femur fractures: an overview of treatment. Orthopedics 1993;16(2):183-90.
9. Porat S, Milgrom C, Nyska M, Whisler JH, Zoltan JD, Mallin BA. Femoral fracture treatment in head-injured children: use of external fixation. Journal of Trauma-Injury Infection & Critical Care 1986;26(1):81-4.
10. Hedin H, Borgquist L, Larsson S. A cost analysis of three methods of treating femoral shaft fractures in children: a comparison of traction in hospital, traction in hospital/home and external fixation. Acta Orthopaedica Scandinavica 2004;75(3):241-8.
11. Gallagher C. Applying quality improvement tools to quality planning: pediatric femur fracture clinical path development. Journal for Healthcare Quality 1994;16(3):6-14.
12. Buechsenschuetz KE, Mehlman CT, Shaw KJ, Crawford AH, Immerman EB. Femoral shaft fractures in children: traction and casting versus elastic stable intramedullary nailing. Journal of Trauma-Injury Infection & Critical Care 2002;53(5):914-21.
13. Flynn JM, Luedtke LM, Ganley TJ, Dawson J, Davidson RS, Dormans JP, et al. Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. Journal of Bone & Joint Surgery - American Volume 2004;86-A(4):770-7.
14. Ferguson J, Nicol RO. Early spica treatment of pediatric femoral shaft fractures. Journal of Pediatric Orthopedics 2000;20(2):189-92.
15. Wright JG, Wang EEL, Owen JL, Stephens D, Graham HK, Hanlon M, et al. Treatments for paediatric femoral fractures: a randomised trial. Lancet 2005;365(9465):1153-8.
16. Kuremsky MA, Frick SL. Advances in the surgical management of pediatric femoral shaft fractures. Current Opinion in Pediatrics 2007;19(1):51-7.
17. Domb BG, Sponseller PD, Ain M, Miller NH. Comparison of dynamic versus static external fixation for pediatric femur fractures. Journal of Pediatric Orthopedics 2002;22(4):428-30.
18. Matzkin EG, Smith EL, Wilson A, Murray PC. External fixation of pediatric femur fractures with cortical contact. American Journal of Orthopedics 2006;35(11):498-501.
19. Ligier JN, Metaizeau JP, Prevot J, Lascombes P. Elastic stable intramedullary nailing of femoral shaft fractures in children. Journal of Bone & Joint Surgery - British Volume 1988;70(1):74-7.
20. Ozdemir HM, Yensel U, Senaran H, Mutlu M, Kutlu A. Immediate percutaneous intramedullary fixation and functional bracing for the treatment of pediatric femoral shaft fracture. Journal of Pediatric Orthopedics 2003;23(4):453-7.
21. Pate O, Hedequist D, Leong N, Hresko T. Implant removal after submuscular plating for pediatric femur fractures. Journal of Pediatric Orthopedics 2009;29(7):709-12.
22. Garner MR, Bhat SB, Khujanazarov I, Flynn JM, Spiegel D. Fixation of length-stable femoral shaft fractures in heavier children: flexible nails vs rigid locked nails. Journal of Pediatric Orthopedics 2011;31(1):11-6.
23. MacNeil JAM, Francis A, El-Hawary R. A systematic review of rigid, locked, intramedullary nail insertion sites and avascular necrosis of the femoral head in the skeletally immature. Journal of Pediatric Orthopedics 2011;31(4):377-80.
24. El Hayek T, Daher AA, Meouchy W, Ley P, Chammas N, Griffet J. External fixators in the treatment of fractures in children. Journal of Pediatric Orthopaedics, Part B 2004;13(2):103-9.
25. Carmichael KD, Bynum J, Goucher N. Rates of refracture associated with external fixation in pediatric femur fractures. American Journal of Orthopedics 2005;34(9):439-44.
26. Sagan ML, Datta JC, Olney BW, Lansford TJ, McIff TE. Residual deformity after treatment of pediatric femur fractures with flexible titanium nails. Journal of Pediatric Orthopedics 2010;30(7):638-43.
27. Rathjen KE, Riccio AI, De La Garza D. Stainless steel flexible intramedullary fixation of unstable femoral shaft fractures in children. Journal of Pediatric Orthopedics 2007;27(4):432-41.
28. Poolman RW, Kocher MS, Bhandari M. Pediatric femoral fractures: a systematic review of 2422 cases. Journal of Orthopaedic Trauma 2006;20(9):648-54.
29. Jencikova-Celerin L, Phillips JH, Werk LN, Wiltrout SA, Nathanson I. Flexible interlocked nailing of pediatric femoral fractures: experience with a new flexible interlocking intramedullary nail compared with other fixation procedures. Journal of Pediatric Orthopedics 2008;28(8):864-73.
30. Sturdee SW, Templeton PA, Dahabreh Z, Cullen E, Giannoudis PV. Femoral fractures in children, is early interventional treatment beneficial? Injury 2007;38(8):937-44.
31. Barlas K, Beg H. Flexible intramedullary nailing versus external fixation of paediatric femoral fractures. Acta Orthopaedica Belgica 2006;72(2):159-63.
32. Wall EJ, Jain V, Vora V, Mehlman CT, Crawford AH. Complications of titanium and stainless steel elastic nail fixation of pediatric femoral fractures. Journal of Bone & Joint Surgery - American Volume 2008;90(6):1305-13.
33. Mani US, Sabatino CT, Sabharwal S, Svach DJ, Suslak A, Behrens FF. Biomechanical comparison of flexible stainless steel and titanium nails with external fixation using a femur fracture model. Journal of Pediatric Orthopedics 2006;26(2):182-7.
34. Mahar AT, Lee SS, Lalonde FD, Impelluso T, Newton PO. Biomechanical comparison of stainless steel and titanium nails for fixation of simulated femoral fractures. Journal of Pediatric Orthopedics 2004;24(6):638-41.
35. Papadokostakis G, Kontakis G, Giannoudis P, Hadjipavlou A. External fixation devices in the treatment of fractures of the tibial plafond: a systematic review of the literature. Journal of Bone & Joint Surgery - British Volume 2008;90(1):1-6.
36. Leet AI, Pichard CP, Ain MC. Surgical treatment of femoral fractures in obese children: does excessive body weight increase the rate of complications? Journal of Bone & Joint Surgery - American Volume 2005;87(12):2609-13.
37. Ramseier LE, Bhaskar AR, Cole WG, Howard AW. Treatment of open femur fractures in children: comparison between external fixator and intramedullary nailing. Journal of Pediatric Orthopedics 2007;27(7):748-50.
38. Ramseier LE, Janicki JA, Weir S, Narayanan UG. Femoral fractures in adolescents: a comparison of four methods of fixation. Journal of Bone & Joint Surgery - American Volume 2010;92(5):1122-9.
39. Wilson NC, Stott NS. Paediatric femoral fractures: factors influencing length of stay and readmission rate. Injury 2007;38(8):931-6.
40. Lee SS, Mahar AT, Newton PO. Ender nail fixation of pediatric femur fractures: a biomechanical analysis. Journal of Pediatric Orthopedics 2001;21(4):442-5.
41. Bar-On E, Sagiv S, Porat S. External fixation or flexible intramedullary nailing for femoral shaft fractures in children. A prospective, randomised study. Journal of Bone & Joint Surgery - British Volume 1997;79(6):975-8.
Legends
Table 1. Medline search strategy
Table 2. Results of the included
studies
Figure 1. Selection of included studies
|

