Address for Correspondence
Prof. Won Yong Shon, MD, PhD.
Dept of Orthopaedics,
Korea University Guro Hospital,
97 Gurodong-gil, Guro-gu,
Seoul 152-703, Korea
Phone: 82-2-2626 1163
Fax: 82-2-2626 1163
Email: shonwy@hotmail.co
Abstract
CLS Spotorno expansion acetabular cup is in use since 1984 for uncemented Metal-Polyethylene (PE) hip arthroplasties. Metal-PE articulations are notoriously known to wear and lead to failure of Total Hip Arthroplasty (THA). However, catastrophic breakage of expansion acetabular cup is rare. We report the first case of expansion cup breakage for metal-PE articulation. A 74-year-old male who underwent bilateral THA using metal expansion acetabular cups in 1991, presented with right hip pain and inability to walk, after 15 years. Post-operatively patient is able to ambulate with crutch aid. We stress on importance of regular follow-up to identify early PE wear and prevent secondary catastrophic failure of THRA. A comprehensive review of similar cases has been included.
J.Orthopaedics 2011;8(3)e3
Keywords:
CLS expansion cup; catastrophic failure; revision hip arthroplasty; osteolysis.
Introduction:
Polyethylene (PE) liner wear and secondary osteolysis is a well established mechanism of failure for metal-PE total hip replacement arthroplasty (THRA) [1-3]. However, extensive liner wear leading to catastrophic breakage of metallic acetabulum shell is a rarity. A handful of cases are reported with fracture of various designs of metal acetabular shell in the conventional metal-PE, ceramic-PE and the most recent ceramic-ceramic articulations [Table-I].
CLS Expansion Acetabular cup was introduced by Spotorno in 1984 based on the concept of biologic fixation. Since its inception, it has been widely used for treatment of various hip pathologies including Congenital Hip Disease, Coxarthritis and Osteonecrosis [15, 26, 27]. Recent studies from Europe and Asia, have reported high, long term survivorship of this implant in THRA performed over last 2 decades [15,17,25,26]. Failure cases have been associated with polyethylene (PE) wear and osteolysis and due to design, thinness and elasticity of the expansion cup [15, 25, 26]. However, a case of catastrophic rupture of the expansion shell in a ceramic-PE bearing has only been reported once [11]. To the best of our knowledge, this is the first case of expansion cup breakage in a metal-PE articulation, in a patient with bilateral expansion cups.
Patient Sex/Age. Reference |
Bearing Surface & Primary Acetabular Cup Design. |
Duration In Situ. |
Clinical Symptom & Significant Findings at Presentation. |
Follow-up after Index Surgery. |
Treatment of Cup Breakage |
Outcome of Revision surgery |
F/53 Yr,
DDH [13]
1997 |
MOPE. Harris-Galante I Cup |
8 Years |
Progressive start-up pain, Crepitation on walking. Liner dissociation, fractured acetabular shell |
Periodic |
Revision with Acetabular reinforcement ring. |
Pain free hip, walks without aids. |
M/58Yr,
OA [5] 1998 |
COPE. Optifix Acetabular cup (Smith & Nephew) |
7 years |
Squeaking Sound.
Superior migration of head within the acetabulum, no osteolysis. |
Lost to Follow-up |
Modular exchange, except femoral stem. |
NA |
F/29 Yr
JRA. [5]
1998 |
COPE. Optifix Acetabular shell (Smith & Nephew) |
7.5 years |
Severe Hip Pain, Grinding sensation.
Eccentric PE wear with osteolysis in Greater trochanter |
NA |
Modular exchange, except femoral stem. |
NA |
M/71Yr,
AVN [7]:
2003 |
MOPE. Harris-Galante Titanium Cup |
12 years |
Persistent hip pain, Clicking sound. Eccentricity of head, bony deficiency at superior wall of left acetabulum |
Irregular Follow-up |
Modular exchange with a 150 lipped liner. |
Pain free and walks with one crutch. |
M/49 Yr [6]:
2008 |
COPE. Richards Optifix acetabular cup 56mm (Smith & Nephew) |
16 years |
Multiple hip dislocations.
Peri-prosthetic osteolysis, complete wear through of PE liner. Cup abduction angle of 550. |
Lost to Follow-up |
NA |
NA |
M/85 Yr
OA [8]:
2009 |
MOPE. Depuy profile Cup |
18 years |
Left anterior hip pain. Eccentric head position, large osteolytic defect in supra acetabular bone. |
Lost to Follow-up |
Complete Revision with bone grafting of osteolytic defect. |
Early post-op death due to cardiac insult. |
F/67 Yr
OA [9]:
2009 |
COC. Osteonics Secure fit HA. |
2 Years |
Pain & Crepitation. Insert fracture and metal shell penetration |
Periodic Follow-up |
Acetabular reinforcement & cross linked PE. |
No marked wear until 7 post revision years. |
M/33 Yr,
Bilateral AS [10]:
2007 |
MOPE. HGP-I acetabular cup. |
5 Years |
Right hip pain, Inability to bear weight. Peri-prosthetic osteolysis and loosening present |
Not mentioned |
Complete revision with acetabular reinforcement ring. |
Walks with a crutch, shoe raise and a slight Trendelenberg gait. |
M/38 Yr
JRA [12]:
2009 |
COPE. Optifix cup (Smith & Nephew). |
14 years |
Left hip pain radiating to groin.
Extensive PE wear with positive Bubble Sign[14] |
Lost to follow-up. |
Complete revision THRA. |
Walks without support, no limp, pain free ROM. |
F/ 50 Yr,
Bilateral AVN[11] 2010 |
COPE. Bilateral CLS Spotorno Expansion cups (Centerpulse, Switzerland). |
Left - 11 years.
Right – In-situ till reported. |
Pain in hip & inability to bear weight on left hip Left: Superior dislocation of ceramic head, Inclination 600. Extensive peri-prosthetic osteolysis. Right: in-situ, inclination 440. |
Not Mentioned |
Complete revision with acetabular reinforcement. |
Returned to previous level of activity, walks with support and painless ROM. |
M/ 74 Yr,
Bilateral AVN [Our Case] |
MOPE. Bilateral CLS Spotorno Expansion cups (Protek AG, Bern). |
Right – 15 years.
Left – In-situ till date. |
Right hip pain & acute inability to bear weight. Severe peri-acetabular osteolysis on right hip. Superior migration of metal head with rupture of cranial half of extension cup. Inclination 460 on right, 540 on left. |
Lost to follow-up |
Resection Arthroplasty with Cement insertion. |
At latest follow-up, patient walks with a crutch, pain free right hip. |
Abbreviations:
PE: Polyethylene.
COPE: Ceramic Head On Polyethylene Liner.
MOPE: Metal Head On Polyethylene Liner.
COC: Ceramic Head On Ceramic Liner
AS: Ankylosing Spondylitis.
DDH: Developmental Dysplasia of Hip.
OA: Osteoarthritis.
JRA: Juvenile Rheumatoid Arthritis.
AVN: Avascular Necrosis.
ROM: Range of Motion.
NA: Not Available
Case:
A 74 year male who was diagnosed with bilateral, steroid induced Avascular Necrosis (AVN) of femoral heads underwent bilateral metal on polyethylene (PE) THRA at our hospital in May 1991. The index implants on right hip were a 52 mm Spotorno CLS expansion cup (Protek AG, Bern), standard PE liner, 28 mm Co-Cr femoral head and a proximally porous coated femoral stem (Zimmer, Warsaw, Indiana). THRA on left hip was performed 15 days later using a 50 mm CLS expansion cup (Protek AG, Bern), standard PE liner, 28mm Co-Cr femoral head and a proximally porous coated cemented femoral stem (Zimmer, Warsaw, Indiana). Patient did well until his 5th year follow-up in 1996 and then lost to follow-up. Hip radiographs done in 2001 demonstrated well placed bilateral hip prosthesis with periacetabular osteolysis, more on the right compared to left side. Cup inclination angle at that visit were 460 on right and 540 on left. There was no acetabular or femoral loosening. Patient was able to walk without support at that time.
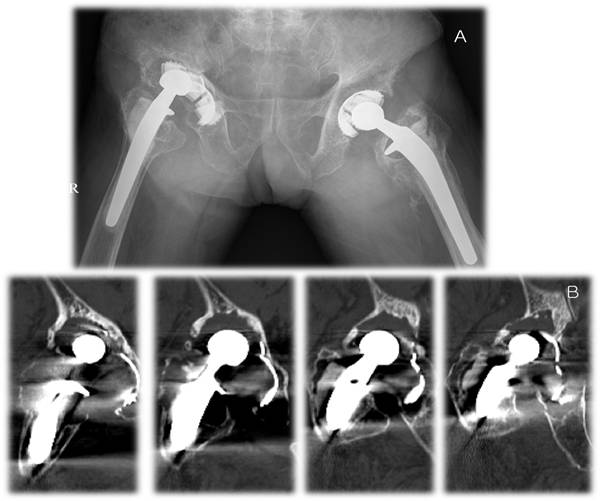
In October 2005, patient returned with pain and progressive inability to bear weight on right hip. Hip radiographs revealed extensive periacetabular osteolysis in DeLee and Charnley’s Zone I, II & III [18] and rupture of cranial half of acetabular cup with superolateral migration of the femoral head on right side. The left hip implant was in situ with mild periacetabular osteolysis without loosening. The cup inclination was 540 on left hip. There was no loosening of the femoral stem on either hip. A diagnosis of right metallic expansion shell rupture was established and a revision arthroplasty was recommended. However, the patient denied revision surgery and preferred wheel chair ambulation until November 2009, when he presented with severe right hip pain. There was no history of fall or trauma. Patient was unable to walk and there was a painful limitation of range of motion (ROM) on the right hip. The ROM on left hip was complete and pain free. Evaluation of radiographs revealed a worsened right metallic acetabular shell fracture with a huge osteolytic defect in the superior rim of acetabulum. Femoral head was in direct contact with the iliac wing through the ruptured acetabular shell (Fig Ia). All radiographic findings were confirmed on Pelvic CT scans (Fig Ib). There was no loosening of femoral stem. The left hip implant was intact in-situ with mild periacetabular osteolysis.
Preoperatively, treatment options in form of complete revision, modular component revision and resection arthroplasty were offered. Pros and Cons of all modalities including that of resection arthroplasty were discussed with the patient and a right sided revision with acetabular reconstruction and exchange of the PE liner was advised. However, patient decided on resection arthroplasty, seeking a pain-free hip with crutch ambulation.
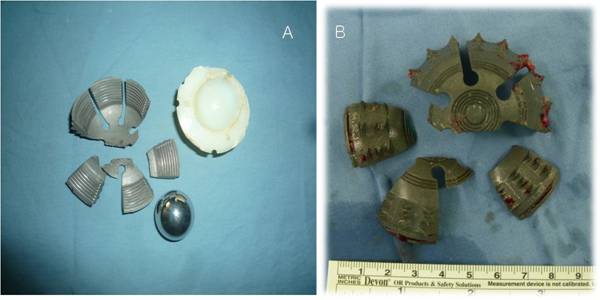
Intra-operatively, extensive and severe metallosis with blackening of hip capsule was found while approaching the right hip through a posterolateral incision. The intact metal femoral head was lying in a huge osteolytic defect in the roof of acetabulum. Cranial rim of the liner showed thinning out due to excessive PE wear (Fig 2a). Extensive osteolysis with secondary rupture of the cranial half of acetabular shell was seen. 3 broken wings and the intact caudal half of the expansion cup were removed carefully (Fig 2b). The femoral prosthesis did not show loosening but had to be removed. Thorough wound irrigation was done and bone cement on the acetabular as well as femoral side was lodged (Fig 3). Meticulous hemostasis was achieved and layer wise closure was performed securing a negative suction drain in situ.
Post-operatively, partial weight bearing using crutches was started from 3rd day. At latest follow-up, patient is gratified with the surgical and rehabilitative outcome and is able to walk with one crutch without hip pain.
F(1)
F(2)

F(3)
Discussion :
The expansion cup, contrived by Spotorno in 1984 is a hemispherical acetabular shell made up of 6 titanium alloy (Ti6A17Nb) wings united at the pole. Each wing has 3 rows of elevated teeth micro-structured on its outer surface to encroach on the native acetabulum providing primary cementless fixation and rotational stability. Secondary fixation is achieved by osteointegration between acetabular subchondral bone and the outer titanium surface [20,21]. The inner surface is threaded to firmly grip the PE liner in-situ to provide an additional rotational stability. The design of the expansion cup is not rigid to match with the contour and mechanics of native acetabulum and this minimizes the relative movement between implant and pelvis [11]. The expansion cup needs to be oriented relatively vertical to achieve complete bony coverage for a stable fixation [27]. Additionally, the potential gap between the wings of expansion cup favors passage of wear particles to the metallic shell [15].
In our patient, the left hip THRA performed at a similar time, using the same components, served as a matched control for comparison. The differences between the 2 sides were presence of severe osteolysis, 52 mm expansion cup, an abduction angle of 460 on right compared to mild osteolysis, 50mm cup size and an inclination angle of 570 on left. We believe that the severe osteolytic lesions on right with loss of bony acetabular support lead to the catastrophic fatigue breakage of CLS cup in our patient. The extensive osteolysis was secondary to severe PE liner wear in its cranial pole (Fig 2a, 2b). The possibility of fatigue fracture attributed to its elasticity and thinness is also reported by Kim et al [15]. The metallic femoral head was displaced superolaterally in the osteolytic defect. In another similar case, head was displaced superiorly [11]. The direction of wear and migration of head is possibly explained by the finding that when wear, a local mechanical factor precipitates osteolysis, the femoral head will move superolaterally, superomedially when creep plays a major role and superiorly with a combination of creep and wear [24].
Unlike the report for breakage of expansion cup in ceramic-PE articulation [11], where the left cup with an inclination angle of 600 broke, the cup which experienced catastrophic breakage was angled at 460 in our case. Needham et al [6] also reported an abduction angle of 550 associated with a breakage of Richards Optifix acetabular cup (Smith & Nephew Richards, Memphis, Tennessee). In contrast, the cup on left is more vertical than right (540), which is still intact. However, our review of literature did not retrieve any study establishing a definite role of cup position in CLS Spotorno expansion cup breakage.
Cases of catastrophic breakage of acetabular components other than the CLS expansion design have been reported for metal-PE articulations [4,7,8,10,13,16]. Of note is breakage of Harris-Galante Porous (HGP) cups which is usually attributed to a suboptimal liner locking mechanism [7, 10, 13]. Cases with catastrophic cup breakage for ceramic-PE [5,6,11,12] and Ceramic-Ceramic [9] THRA have also been reported in English literature (Table I). However, irrespective of the type of bearing surface, presence of extensive periacetabular osteolysis is common to most of the reported cases [5,6,7,8,10,11]. An irregular or lost to follow-up for all such cases [5,6,7,8,12] is also noteworthy. Indeed, our case also reports a presence of severe osteolysis in roof of acetabulum and a long follow-up lag after five years of index surgery.
Clinically, patients with acetabular shell rupture present with an array of descriptions ranging from squeaking and clicking sounds, grinding sensation or crepitation while walking and on passive motions of affected hip. Additionally, they may also present with history of multiple hip dislocations and persistently progressive hip pain with radiation to either thigh or knee (Table I). Radiographic signs of excessive wear and metallosis including eccentric position of femoral head, a dissociated liner, progressive osteolytic lesions in the roof of acetabulum and the bubble sign [14] should be suspiciously seen as indicators of future catastrophic acetabular failure. Risk factors for catastrophic failure include male gender, younger patient with high activity, metal compared to ceramic head, femoral head size, use of conventional PE, PE thinness, gamma-in-air sterilization of PE, cup abduction angle of >450, suboptimal locking mechanism and non-articular back side wear [5, 6, 22, 23]. Presence of any of these should be identified on follow-up visits to prevent accelerated wear and its complications.
Clinical course in our patient was dramatic: patient presented with hip pain and acute inability to bear weight associated with superolateral dislocation of femoral head on radiographs. Irregular follow-up visits did not allow a timely diagnosis of accelerated wear and osteolysis, which lead to fatigue breakage of cup. The end point was a resection arthroplasty rather than a total revision surgery respecting patient’s decision. At the most recent follow-up patient is satisfied with the outcome and is able to walk with support. Although we were able to provide the outcome which patient sought for, we strongly feel that a regular yearly follow-up even after many years of index surgery would have avoided resection arthroplasty. Similar to results of the American Association of Hip and Knee Surgeons Member’s survey [19], we also recommend, long term annual or biennial post-THRA surveillance.
Conclusion:
Our case represents a very late and uncommon complication of the conventional metal on polyethylene THRA in form of accelerated PE wear leading to catastrophic breakage of the metallic expansion acetabular shell and superolateral dislocation of femoral head. This greatly hampered the ability of a patient to ambulate without support, who was doing functionally well for last 15 years. The whole catastrophe would have been avoided simply by a regular surveillance and timely diagnosis of PE wear and osteolysis. Surgeons can resort to a less extensive procedure like isolated PE liner and femoral head exchange instead of an extensive revision THRA or a morbidity associated resection arthroplasty. This emphasizes the significance of regular yearly follow-up to identify clinical and radiological signs of PE wear and osteolysis, even after many years of a THA.
Reference :
1. Skinner HB. Ceramic bearing surfaces. Clin Orthop Relat Res 1999:83.
2. Clarke IC, Gustafson A. Clinical and hip simulator comparisons of ceramic-on-polyethylene and metal-on-polyethylene wear. Clin Orthop Relat Res 2000:34.
3. Urban JA, Garvin KL, Boese CK, et al. Ceramic-on-polyethylene bearing surfaces in total hip arthroplasty. Seventeen to twenty-one-year results. J Bone Joint Surg Am 2001;83-A:1688.
4. Berry DJ, Barnes CL, Scott RD, et al. Catastrophic failure of the polyethylene liner of uncemented acetabular components. J Bone Joint Surg Br 1994;76:575.
5. Simon JA, Dayan AJ, Ergas E, et al. Catastrophic failure of the acetabular component in a ceramic-polyethylene bearing total hip arthroplasty. J Arthroplasty 1998;13:108.
6. Needham J, Burns T, Gerlinger T. Catastrophic failure of ceramic-polyethylene bearing total hip arthroplasty. J Arthroplasty 2008;23:627.
7. Huang KY, Liu HC, Hou SM. Wear-through of metal-backed acetabular shell in total hip arthroplasty. J Formos Med Assoc 2003;102:334.
8. Sherman RA, Damron TA. Penetration of a metallic femoral head through the acetabular shell. J Arthroplasty 2009;24:1143 e7.
9. Baba T, Shitoto K. A case of insert fracture and metal shell penetration by the inner head after ceramic-on-ceramic THA. Eur J Orthop Surg Traumatol 2009;19:109.
10. Lakdawala A, Konchuwalla A, Gad-el Rab R. Penetration of the head of a femoral prosthesis through the metal shell of a Harris-Galante type-I acetabular component: an unusual complication. Internet J Orthop Surg 2007;4:2.
11. Mariconda M, Silvestro A, Mansueto G, et al. Complete polyethylene wear-through and secondary breakage of the expansion cup in a ceramic-polyethylene total hip arthroplasty. Arch Orthop Trauma Surg 2010;130:61.
12. Malizos K, Roidis NT, Poultsides L, et al. Protrusio of a ceramic femoral head through the acetabular metallic shell, extensive metallosis and 'bubble sign'. Orthopedics 2009;32:128.
13. Trousdale RT, Berry DJ, Jacobs J, et al. Fracture of an acetabular component inserted without cement. A case report. J Bone Joint Surg Am 1997;79:901.
14. Su EP, Callander PW, Salvati EA. The bubble sign: a new radiographic sign in total hip arthroplasty. J Arthroplasty 2003;18:110.
15. Kim YG, Kim SY, Kim SJ, et al. The use of cementless expansion acetabular component and an alumina-polyethylene bearing in total hip arthroplasty for osteonecrosis. J Bone Joint Surg Br 2005;87:776.
16. Engh CA, Jr., Hopper RH, Engh CA, et al. Wear-through of a modular polyethylene liner: four case reports. Clin Orthop Relat Res 2001:175.
17. Modrego FJ, Molina J. [Self-expanding cup CLS. 10 years results]. Rev Fac Cien Med Univ Nac Cordoba 2004;61:7.
18. DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res 1976:20.
19. Teeny SM, York SC, Mesko JW, et al. Long-term follow-up care recommendations after total hip and knee arthroplasty: results of the American Association of Hip and Knee Surgeons' member survey. J Arthroplasty 2003;18:954.
20. Blaha DJ, Spotorno L, Romagnoli S. CLS press-fit total hip arthroplasty. Tech Orthop 1991;6:80.
21. Spotorno L. The CLS system—a 16-year review. An emerging gold standard for uncemented hip replacement?. Int Orthopedics 2000;24:1.
22. Wan Z, Boutary M, Dorr LD. The influence of acetabular component position on wear in total hip arthroplasty. J Arthroplasty 2008;23:51.
23. Patil S, Bergula A, Chen PC, et al. Polyethylene wear and acetabular component orientation. J Bone Joint Surg Am 2003;85-A Suppl 4:56.
24. Murray DW, O'Connor JJ. Superolateral wear of the acetabulum. J Bone Joint Surg Br 1998;80:197.
25. Rozkydal Z, Janicek P, Tomas T, et al. [Long-term results of the CLS acetabular cup in primary total hip replacement]. Acta Chir Orthop Traumatol Cech 2009;76:90.
26. Rozkydal Z, Janicek P, Smid Z. Total hip replacement with the CLS expansion shell and a structural femoral head autograft for patients with congenital hip disease. J Bone Joint Surg Am 2005;87:801.
27. Orozco R, Koch PF, Giros J, et al. Provisional results of the CLS cup using IDES. Int Orthop 1994;18:363. |

