|
Abstract:
Purpose : The purpose of this study is to investigate and analyze accompanying shoulder lesions according to the type of anteroinferiallabral lesion in the recurrent anterior shoulder dislocation patientsby using radiologic and arthroscopic findings.
Methods : 82 patients with recurrent anterior shoulder dislocation treated with arthroscopic operation were included in this study. We classified anteroinferiorlabral lesions based on the presence of bony Bankart lesion and chronocity of capsulolabral complex and evaluated concomitant shoulder lesions (rotator cuff lesion, biceps lesion, cystic lesion of the humeral head, Superior labrum from anterior-to-posterior(SLAP) lesion,Acromioclavicular(AC) joint arthritis and Hill-sach lesion according to the classified subgroups.
Results :The bony Bankart lesion group showed six cases of SLAP lesions (17.1%), eight cases of cystic change lesions (22.8%), and 11 cases of rotator cuff lesions (31.4%).The group with no bony Bankart lesion featured two cases of bicep lesions (6.3%), three cases of cystic change lesions (6.3%), three cases of rotator cuff lesions (6.3%). These lesions also showed significant difference between two subgroups according to the presence of bony Bankart (p=0.044, 0.042, 0.034, respectively). However,there was no significant difference in the prevalence of concomitant shoulder lesions between two subgroups according to the chronocity of capsulolabral complex (p>0.05).
Conclusion : SLAP lesions, rotaor cuff lesions and cystic lesion of humeral head were more prevalent in the bony Bankart group compared with soft-tissue Bankart group.
Keywords:
shoulder, labrum, Bankart lesion, recurrent dislocation d
J.Orthopaedics 2012;9(1)e12
Introduction:
The shoulder is one of the most versatile joint in the human body. However, motions in multi- plane causes the joint vulnerable to instability. Anterior shoulder dislocation occurs in approximately 0.7% for men and 0.3% for women up to the age of 70[1].Hovelius reported the prevalence of shoulder dislocation to be 1.7%[2]. Anterior shoulder instability can be classified in magnitude by subluxation or dislocation; by duration as acute, recurrent, or chronic; and by its etiology as traumatic or atraumatic. The most common cause of anterior shoulder instability is a traumatic injury that creates an initial dislocation, which is often associated with the anteroinferiorglenoid labrum and anteroinferiorglenohumeral ligament. Detachment of the labrum from the anterior rim of the glenoid cavity is an essential lesion in recurrent dislocations. In this case, the only rational treatment is to reattach the glenoid ligament (or the capsule) to the bone from which it has been torn. Most authors agree that a Bankart lesion is the most commonly observed pathologic lesion in recurrent subluxation or dislocation of the shoulder. Although the Bankart lesion has been described as the essential lesion in patients with anterior shoulder instability, biomechanical and clinical studies have demonstrated that a wide variety of pathologic changes occur in patients with these lesions[2,3,4,5].In addition, there are many studies on capsulolabral lesions in recurrent anterior shoulder dislocation.[7-12] However, few studies have reported on the concomitant pathologic changes of the shoulder in recurrent anterior shoulder dislocation[6-7]. Furthermore, there is no study to date on concomitant pathologic changes of the shoulder according to the type of anteroinferiorlabral lesions in recurrent anterior shoulder dislocation. The purpose of this study is to compare concomitant pathologic changes of the shoulder according to the type of anteroinferiorlabral lesions in recurrent anterior shoulder dislocation, particularly according to the chronologic classification of the capsulolabral complex and the presence of a bony Bankart lesion.
Materials and methods:
Study Design
After approval was obtained from the institutional review board, we conducted a search of the senior authors database. We reviewed 140 patients suffering from recurrent anterior shoulder dislocation who had received preoperative Magnetic Resonance Imaging (MRI) or Magnetic Resonance Angiography (MRA) and surgery performed by the senior author between January 2003 and April 2010. The inclusion criteria were: 1) the first dislocation was caused by a traumatic event; 2) patients had at least three recurrences of traumatic anterior shoulder dislocation; 3) the latest dislocation had occurred at least three months prior to the time of surgery; 4) radiologic evaluation was carried out up to two weeks before the surgery; 5) medical records had been satisfactorily completed; 6) the presence of an anterior inferior labral lesion that could be classified by a radiologist and surgeon according to its chronocity; and 7) a less than 25% bony defect re-evaluated by MRI or MRA and arthroscopic findings. Among the 140 patients, 103 were deemed as suitable subjects for this study.
Exclusion criteria were: 1) revision of shoulder operation; 2) previous shoulder surgery; 3) multidirectional instability; and 4) a difference between the operational and radiological findings. After the exclusion criteria had been applied, 82 patients were finally selected as subjects for this study.
We divided the subjects into four groups according to chronocity, degree of anteroinferiorlabral lesion, and the presence of a bony Bankart lesion. First, the chronologic classification of the capsulolabral complex was modified using the Harbermyerclassification[10]. Classic Bankart lesions and Perthes lesions were classified as being early stage in the capsulolabral complex. Double lesions, triple lesions, and anterior labroligamentousperiosteal sleeve avulsion (ALPSA) lesions were classified as late lesions. The groups were also divided by the presence or absence of a bony Bankart lesion. All the subjects were classified into four groups. Group one comprised early capsulolabral lesions without a bony Bankart lesion. Group two featured early capsulolabral lesions with a bony Bankart lesion. Group three comprised late capsulolabral lesions without a bony Bankart lesion. Group four featured late capsulolabral lesions with a bony Bankart lesion. In addition, we separately evaluated the difference according to chronocity, degree of anteroinferiorlabral lesion, and the presence of a bony Bankart lesion (Fig. 1).
We also set up pathologic changes of shoulder that are thought to be affected by recurrent anterior shoulder dislocation such as 1) bicep lesion; 2) Superior labrum from anterior-to-posterior(SLAP) lesion; 3) Acromioclavicular (AC) joint arthritis; 4) cystic lesion of the humeral head; 5) Hill-Sachs lesion; and 7) rotator cuff lesion.
In order to evaluate the bicep lesions, we considered them as bicep tears, subluxation, and dislocations. With regard to the SLAP lesions, we only evaluated SLAP type II, which was diagnosed and confirmed by arthroscopic findings. For the evaluation of the AC joint arthritis, this was considered to be present upon finding direct tenderness of the AC joint on physical examination and MRI findings such as increased signal intensity on the AC joint and joint fluid swelling. Cystic lesions of the humeral head were evaluated by MRI and differentiated from diffuse bony edema. The rotator cuff condition was evaluated by tear type as articular-sided, bursal-sided, or full thickness, and by location as either posterosuperior or anterosuperior.
Data analysis
Through a review of the medical records, we evaluated the sex and age of the subjects at the time of their first injury. In addition, the number and frequency of dislocation events were checked. We also evaluated the frequency of accompanying lesions that showed a statistically significant difference among the groups. Statistical evaluations used SAS version 9.2 (SAS Instiute, Cary, North Carolina) and all statistical analyses were performed by a specialized biostatistician. The level of significance was set at 0.05. Statistical difference between the four groups with regards to continuous and discrete variables was evaluated by Kruskal-Wallis analysis and the Chi square test, respectively. Statistical difference between the two groups divided by the presence of a bony Bankart lesion, and the chronocity of the lesion with regards to discrete variables (biceps lesions, AC joints arthritis, cystic changes of the humeral head, and rotator cuff lesions), were evaluated using the Chi square test.
Results
Among the 82 patients, 81 cases were male, one was female, and the mean age was 30.9 years old (range of 18-53 years). There were no statistically significant differences in the frequency of dislocation, age at the initial dislocation, or delayed time interval between the initial dislocation and surgery among the groups (p>0.05) (Table 1). A comparison of the four groups with regards to the discrete variables (bicep lesions, SLAP lesions, cystic changes of the humeral head, Hill-Sachs lesions, and rotator cuff lesions) showed a statistically significant difference for factors of SLAP lesions, cystic changes of the humeral head, and rotator cuff lesions among the groups (Table 2). With regards to SLAP lesions, two cases were identified (5.1%) in group one; five cases (16.6%) in group two; no cases (0%) in group three; and one case (20%) in group four. Concerning cystic lesions, there were two cases (5.1%) in group one; six cases (20%) in group two; one case (12.5%) in group three; and two cases (40%) in group four. With regards to AC joint arthritis, there was only one case (2.5%) in group one, with no cases reported in the other groups. For the Hill-Sachs lesions, there were 34 cases (87.1%) in group one, 26 cases (86.6%) in group two, seven cases (87.5%) in group three, and four cases (80%) in group four.
When comparing the two groups divided by the presence of a bony Bankart lesion, for the discrete factors (bicep lesions, AC joint arthritis, cystic changes of the humeral head, and rotator cuff lesions), a statistically significant difference was found in this study for the factors of SLAP lesions, cystic changes of the humeral head, and rotator cuff lesions (p=0.044, p=0.034, p=0.042, respectively). The bony Bankart lesion group featured six cases of SLAP lesions (17.1%), eight cases of cystic change lesions (22.8%), and 11 cases of rotator cuff lesions (31.4%). However, the group with no bony Bankart lesion showed two cases of bicep lesions (6.3%), three cases of cystic change lesions (6.3%), three cases of rotator cuff lesions (6.3%) (Table 3).
When comparing the two groups divided by the chronicity of soft tissue Bankart lesions, there was no significant difference regarding discrete factors between the two groups (p>0.05)(Table 4). We evaluated the combined lesions that showed a significant difference according to the group. There were five cases of three lesions (rotator cuff lesion + SLAP lesions + cystic lesion); three cases of two lesions (rotator cuff lesion + SLAP lesion, SLAP lesion + cystic lesion, rotator cuff lesion + cystic lesion); and two cases of a single lesion (rotator cuff lesion, cystic lesion, SLAP lesion) in the bony Bankart lesion groups. In the no bony Bankart lesion group, there were no cases of triple lesions; one case of double lesions; and five cases of a single lesion. In the case of triple and double lesions, the bony Bankart lesion groups showed more prevalence compared with no bony Bankart lesion groups, which was a statistically significant difference. However, in case of a single lesion, the no bony Bankart lesion group showed more prevalence compared with the bony Bankart lesion group, which was a statistically significant difference (Table 5). Table 6 shows the distribution of rotator cuff lesions according to the type listed. Eight cases of articular-sided rotator cuff tears were found in group two; two cases were found in group four; and one case was found in group one. There were no cases ofbursal-sided rotator cuff tears or full thickness rotator cuff tears.
In this study, we subdivided anterior shoulder instability according to bony lesions and the chronocity of soft tissue lesions and compared the associated difference in shoulder lesions between the groups.
There was no difference in the chronology of soft tissue Bankart lesions in the glenohumeral lesions, but a significant difference was found with the presence of a bony lesion in the glenohumeral lesions. In addition, humeral cystic changes, rotator cuff tears, and SLAP lesions were more prevalent in the bony Bankart lesion group compared with the soft-tissue Bankart group.
A Bankart lesion is just one of the findings in the pathologic studies of patients with recurrent shoulder dislocation[5,13-14]. However, patients with recurrent shoulder instability often present an osseous injury of the glenoid and humeral head as well[15].Understanding and appropriately addressing irregularities in the osseous architecture of the glenohumeral joints is therefore critical to the overall success of surgical repair for the treatment of glenohumeralinstability. The integrity of the osseous architecture of the glenoid has recently been highlighted as one of the most important factors in the success of surgical repair. After the initial traumatic shoulder dislocation, an associated glenoid rim fracture or attritional bone injury may compromise the static restraints of the glenohumeral joint, making further instability more likely. Most literaturehas focused on the evaluation of bony lesions of more than 20-25% because they cause instability and failure after surgery if appropriate treatment has not been given. Lesions of less than 20-25% have been underestimated and their importance in the perioperative period has not been evaluated in this study.
Our study showed a high prevalence of rotator cuff tears in the bony Bankart lesion group compared with the soft-tissue Bankart lesion group. Other studies have suggested that a rotator cuff tear may develop in an elderly person with recurrent shoulder instability at an incidence rate of approximately 15-40%[6]. It is impossible to establish whether a lesion of the capsular-labral complex or rotator cuff causes or follows a dislocation, there is a strong relationship between recurrent shoulder instability and rotator cuff tear. The strength of relation is higher in the cases where repetitive dislocation occurs more than seven times. Yiannakopoulos et al.[6] compared the spectrum of intra-articular lesions in acute and chronic anterior shoulder instability. They proposed that the difference between acute and chronic instability is a result of the intervention of the healing response in repetitive dislocations or subluxation episodes, which leads to additional injuries. In addition, they suggest that only partial undersurface cuff tears occur. A strong correlation between an instability episode and rotator cuff tears is evident in patients aged from 40 to 60 years old. In our study, we demonstrated that rotator cuff tear developed with an incidence rate of 17.0%among the traumatic recurrent shoulder dislocation patients. This incidence rate was the similar to those found in other studies. Furthermore, the types of rotator cuff lesions were partial thickness tear and articular-sided tear. A major difference between our study and other studies is that the bony Bankart lesion group showed a higher incidence of rotator cuff tears.
Intraosseous cysts may develop secondarily as a result of elevated intra-articular pressurethe impact between opposing osseous surfaces, or micro-avulsion at tendinousinsertions. There have been no studies on cystic lesions of the humeral head to date in light of patients with recurrent shoulder dislocation. In current literature, 8 cases of cystic lesion were found in the bony Bankart lesion group and 3 cases of cystic lesion were founded in the no bony Bankart lesion group. We found that cystic changes of the humeral head were more prevalent in the bony Bankart lesion group compared with the no bony Bankart lesion group. The clinical importance of a cystic lesion of the humeral head in the anterior shoulder dislocation is unclear and we are unable to determine either the meaning or importance of humeral cystic changes in this study. However, we infer that a bony Bankart lesion may affect the cystic lesion of the humeral head.
SLAP lesions were reported as lesions that occur with traumatic anterior shoulder instability. Kim et al.[3]evaluated the prevalence of accompanying lesions between primary and recurrent anterior dislocation in the shoulder. They studied 28 cases of SLAP lesions (25.2%) and 16 cases of SLAP type II lesions(14.4%) among 111 recurrent shoulder dislocation patients. In the current literature, 6 cases of SLAP type II lesion (17.1%) were found in the bony Bankart lesion group and 2 cases of SLAP type II lesion (4.2%) were found in the no bony Bankart lesion group. We also found that SLAP lesions were more prevalent in the bony Bankart lesion group and suggest that a bony Bankart lesion may be related to SLAP lesions.
Interestingly, the bony Bankart lesion group showed not only significant bicep lesions, cystic changes, and rotator cuff lesions, but also prevalence of triple lesions of the shoulder compared with the no bony Bankart lesion group. On the contrary, the groups with no bony Bankart lesion showed prevalence of a single lesion of the shoulder. This means there may be different pathogenesis of concomitant lesions. One possible explanation for these findings is that: 1) the bony Bankart lesion group may have suffered a greater amount of damage during the initial traumatic event compared with no bony Bankart lesion group, so the group showed a difference of type and overlapping of concomitant shoulder lesion; 2) when the bony Bankart lesion is present, the anterior buttress effect is decreased, so anterior micro-instability will occur unlike in the group without a bony Bankart lesion. This will make the anterior translation a similar mechanism to post-capsule tightness and anterior capsule loosening, so that the contact between the posterosuperior aspect of the labrum and the surface of the rotator cuff facing the glenoid may become pathologic even in non-athletic and normal conditions like internal impingment syndrome. In addition, micro-instability will lead to various shoulder lesions in the patient as time goes on. This study has five main limitations. First, this is a retrospective study so we cannot confirm whether internal impingements, such as rotator cuff tears, humeral head cystic changes, and bicep lesions were the result of recurrent traumatic dislocation events or micro-instability. It is thought to be a starting point for future research rather than a definitive study. Biomechanical studies on the buttress effect of bony fragments and micro-instability are required. Second, we did not evaluate the outcome; this might have provided valuable information and important results regarding small bone fragment fixation. As we had not attempted bony fragment reattachment before 2009, the comparison between the fixation and no-fixation groups could not be included in this study. We plan to carry out a prospective control study on this topic. A third limitation was the non-evaluation of AC joint lesions and the rotator interval index by the arthroscopic operative finding, but only by the radiologic findings. This may have caused some bias in the results. We attempted to select subjects whose radiologic evaluation had been carried out within a period of two weeks prior to surgery in order to reduce the bias of the results.Fourthly, we did not evaluate the lesions according to the degree of the bony Bankart lesions. However, the purpose of this study was to find the difference according to the presence of Bankart lesion and the chronocity of soft tissue, so the degree of the bony Bankart lesion was not included in the study. Finally, the small sample size of groups three and four are additional shortcomings. However, we believe that the sample size for the comparison of the bony Bankart lesions and the chronocity of soft-tissue lesions was adequate.
Conclusion
The prevalence of concomitant shoulder lesions in the case of recurrent shoulder dislocation was affected by the presence of a bony Bankart lesion, but not by the chronology of soft-tissue Bankart lesions. Humeral cystic changes, rotator cuff tears, and SLAP lesions were more prevalent in the bony Bankart lesion group compared with the soft-tissue Bankart lesion group. In addition, the overlapping of concomitant shoulder lesions was more prevalent in the bony Bankart lesion group. In recurrent shoulder dislocation, with even small bony fragments, we try to find the concomitant shoulder lesion. When these lesions are missed, it may give a poor result even t
Reference:
1. Simonet WT, Melton LJ, 3rd, Cofield RH, Ilstrup DM. Incidence of anterior shoulder dislocation in Olmsted County, Minnesota.Clin Orthop Relat Res. 1984; 186: 186-191.
2. Hovelius L. Incidence of shoulder dislocation in Sweden. Clin Orthop Relat Res. 1982; 166: 127-131.
3. Kim DS, Yoon YS, Yi CH. Prevalence comparison of accompanying lesions between primary and recurrent anterior dislocation in the shoulder. Am J Sports Med. 2010; 38(10): 2071-2076.
4. Pouliart N, Marmor S, Gagey O. Simulated capsulolabral lesion in cadavers: dislocation does not result from a bankart lesion only. Arthroscopy. 2006; 22(7): 748-754.
5. Speer KP, Deng X, Borrero S, Torzilli PA, Altchek DA, Warren RF. Biomechanical evaluation of a simulated Bankart lesion. J Bone Joint Surg Am. 1994; 76(12): 1819-1826.
6. Yiannakopoulos CK, Mataragas E, Antonogiannakis E. A comparison of the spectrum of intra-articular lesions in acute and chronic anterior shoulder instability. Arthroscopy. 2007; 23(9): 985-990.
7.Bui-Mansfield LT, Banks KP, Taylor DC. Humeral avulsion of the glenohumeral ligaments: the HAGL lesion. Am J Sports Med. 2007; 35(11): 1960-1966.
8.Fujii Y, Yoneda M, Wakitani S, Hayashida K. Histologic analysis of bony Bankartlesions in recurrent anterior instability of the shoulder. J Shoulder Elbow Surg.2006;15(2):218-223.
9. Gerber C, Nyffeler RW. Classification of glenohumeral joint instability.ClinOrthopRelat Res.2002; 400: 65-76.
10. Habermeyer P, Gleyze P, Rickert M. Evolution of lesions of the labrum-ligament complex in posttraumatic anterior shoulder instability: a prospective study. J Shoulder Elbow Surg. 1999; 8(1): 66-74.
11.Mizuno N, Yoneda M, Hayashida K, Nakagawa S, Mae T, Izawa K. Recurrent anterior shoulder dislocation caused by a midsubstance complete capsular tear. J Bone Joint SurgAm. 2005; 87(12): 2717-2723.
12. Taylor DC, Arciero RA. Pathologic changes associated with shoulder dislocations. Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations.Am J Sports Med. 1997; 25(3) : 306-311.
13. Mizuno K, Nabeshima Y, Hirohata K. Analysis of Bankart lesion in the recurrent dislocation or subluxation of the shoulder. ClinOrthopRelat Res. 1993, 88:158-165.
14. Pappas AM, Goss TP, Kleinman PK. Symptomatic shoulder instability due to lesions of the glenoid labrum. Am J Sports Med. 1983; 11(5) : 279-288.
15. Bigliani LU, Newton PM, Steinmann SP, Connor PM, McLlveen SJ.(1998) Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. Am J Sports Med. 1998; 26(1): 41-45.
Table 1. Demographic data for patient of each Group in the study
Group |
I |
II |
III |
IV |
p-value |
Number (person) |
39 |
30 |
8 |
5 |
|
Mean age (year) |
32.8 |
30.1 |
28.8 |
27.8 |
0.32 |
Sex (Male:Female) |
39:0 |
29:1 |
8:0 |
5:0 |
|
Frequency of dislocation (times) |
4.1 |
5.2 |
4.7 |
4.6 |
0.063 |
Age at initial dislocation (year) |
27 |
27.4 |
24.1 |
22.4 |
0.54 |
Delayed time interval (month) |
76.9 |
45.0 |
65.4 |
64.8 |
0.35 |
Group |
SLAP lesions
(type 2) |
Biceps
lesions |
Cystic lesion
of the humerus |
AC joint
arthritis |
Rotator cuff
lesions |
Hill- sach
lesion |
NB*(47) |
2/47
(4.2%) |
1/47
(2.1%) |
3/47
(6.3%) |
1/47
(2.1%) |
3/47
(6.3%) |
41/47
(87.2%) |
B† (35) |
6/35
(17.1%) |
1/35
(2.8%) |
8/35
(22.8%) |
0/35
(0%) |
11/35
(31.4%) |
33/35
(94.2%) |
p-value |
0.044 |
0.775 |
0.034 |
0.936 |
0.042 |
0.852 |
Table 2.Comparision of shoulder lesion according to the classification
Group |
SLAP lesion
(type 2) |
Biceps lesions |
Cystic lesion
of the humerus |
AC joint
arthritis |
Rotator cuff lesions |
Hii-sach lesion |
I* |
2/39
(5.1%) |
1/39
(2.5%) |
2/39
(5.1%) |
1/39
(2.5%) |
3/39
(7.6%) |
34/39
(87.1%) |
II† |
5/30
(16.6%) |
1/30
(3.3%) |
6/30
(20%) |
0/30
(0%) |
9/30
(30%) |
26/30
(86.6%) |
III‡ |
0/8
(0%) |
0/8
(0%) |
1/8
(12.5%) |
0/8
(0%) |
0/8
(0%) |
7/8
(87.5%) |
IV§ |
1/5
(20%) |
0/5
(0%) |
2/5
(40%) |
0/5
(0%) |
2/5
(40%) |
4/5
(80%) |
p-value |
0.041 |
0.572 |
0.033 |
0.956 |
0.045 |
0.843 |
* earlycapsulolabral lesions without a bony Bankart lesion.
† earlycapsulolabral lesions with a bony Bankart lesion.
‡ latecapsulolabral lesions without a bony Bankart lesion.
§latecapsulolabral lesions with a bony Bankart lesion.
Table 3.Comparision of shoulder lesion according to the presence of bony Bankart lesion
Group |
SLAP lesions
(type 2) |
Biceps
lesions |
Cystic lesion
of the humerus |
AC joint
arthritis |
Rotator cuff
lesions |
Hill- sach
lesion |
NB*(47) |
2/47
(4.2%) |
1/47
(2.1%) |
3/47
(6.3%) |
1/47
(2.1%) |
3/47
(6.3%) |
41/47
(87.2%) |
B† (35) |
6/35
(17.1%) |
1/35
(2.8%) |
8/35
(22.8%) |
0/35
(0%) |
11/35
(31.4%) |
33/35
(94.2%) |
p-value |
0.044 |
0.775 |
0.034 |
0.936 |
0.042 |
0.852 |
*NB:NonbonyBankart lesion
†B:Bankart lesion
Table 4.Comparision of shoulder lesion according to the chronocity of capsulolabral complex.
Group |
SLAP lesions
(type 2) |
Biceps
lesions |
Cystic lesion
of the humerus |
AC joint
arthritis |
Rotator cuff
lesions |
Hill- sach
Lesion |
Early* (69) |
7/69
(10.1%) |
2/69
(2.8%) |
8/69
(11.5%) |
1/69
(1.4%) |
12/69
(17.3%) |
60/69
(86.9%) |
Late† (13) |
1/13
(7.6%) |
0/13
(0%) |
3/13
(23.0%) |
0/13
(0%) |
2/13
(15.3%) |
11/13
(84.6%) |
p-value |
0.368 |
0.438 |
0.472 |
0.934 |
0.588 |
0.874 |
* Early capsulolabral complex
† Late capsulolabraln complex
Table 5.Summary of variables according to location of cuff tear(anterosuprior or posterosuperior) and classification
|
Anterosuperior cuff tear
(Subscapularis) |
Posterosuperior cuff tear |
apt∥ |
bpt¶ |
FT** |
I* |
1 |
2 |
0 |
0 |
II† |
1 |
8 |
0 |
0 |
III‡ |
0 |
0 |
0 |
0 |
IV§ |
0 |
2 |
0 |
0 |
* Early capsulolabral lesions without a bony Bankart lesion.
† Early capsulolabral lesions with a bony Bankart lesion.
‡ Late capsulolabral lesions without a bony Bankart lesion.
§ Late capsulolabral lesions with a bony Bankart lesion.
∥Articular side rotator cuff partial thickness tear.
¶ Bursa side rotator cuff partial Thickness tear.
** Full thickness rotator cuff tear
Table 6.Associated number of lesion between nonbonyBankart group and bony Bankart group
|
Single lesion |
Double lesion |
Triple lesion |
NonbonyBankart group
(47) |
5/47
(10.6%) |
1/47
(2.1%) |
0/47
(0%) |
Bony Bankart group
(35) |
2/35
(5.7%) |
4/35
(11.4%) |
5/35
(14.2%) |
p-value |
0.042 |
0.038 |
0.021 |
Figure 1.
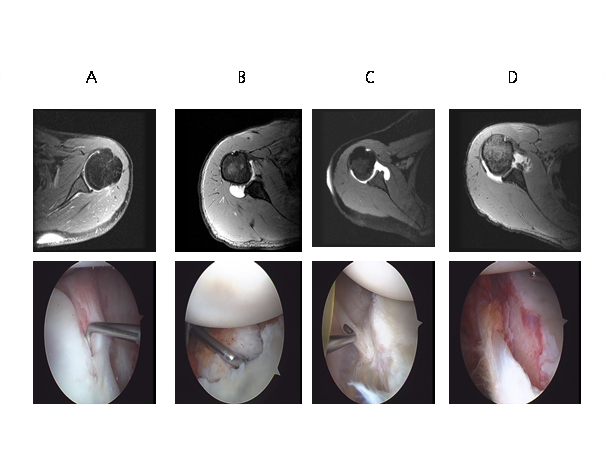
Figure 1. These MRI axial plane image and arthroscopic image demonstrates 4 groups which are divided according to the presence of bony Bankart and chronicity of capsulolabral complex. ( (A) early capsulolabral lesions without a bony Bankart lesion, (B) early capsulolabral lesions with a bony Bankart lesion, (C) late capsulolabral lesions without a bony Bankart lesion, (D) late capsulolabral lesions with a bony Bankart lesion)
|

