| CASE
REPORT |
|
Isolated Ipsilateral Lesser and Greater Trochanteric Hip Fractures without Intertrochanteric Extension: A Case Report.
|
|
N. Watanabe*, Y. Taneda*, H. Iguchi*, T Otsuka*
*Department of Orthopaedics, Kasugai Municipal Hospital, 1-1-1, Takagi-cho, Kasugai City, Aichi, 486-8510, Japan.
**Department of Arthroplastic medicine Nagoya City University Graduate School of Medical Science and Medical School, 1, Kawasumi, Mizuhoku, Nagoya City, Aichi, 467-8601, Japan.
***Department of Orthopedic Surgery Nagoya City University Graduate School of Medical Science and Medical School, 1, Kawasumi, Mizuhoku, Nagoya City, Aichi, 467-8601, Japan.
Address for Correspondence
Nobuyuki Watanabe
Nagoya City University Medical School
1, Kawasumi, Mizuhoku, Nagoya City, Aichi, 467-8601, Japan.
Phone: (81)-(52)-853-8236
Fax: (81)-(52)-842-0266
E-mail: nabearth@med.nagoya-cu.ac.jp
|
|
Abstract:
Isolated Ipsilateral lesser and greater trochanteric hip fracture is extremely rare. As long as we could explore, this would be the first report case of the etiology of the fracture. A 92-year-old male presented right hip pain. He lost his balance and fell over when he was apt to ride on his bicycle. Radiography of the hip has shown avulsion of the lesser trochanter and fracture of the greater trochanter with no apparent intertrochanteric communication. So he was treated conservatively. It is suggested that these fractures happened first, the lesser trochanter fracture occurred as an avulsion fracture when the patient tried not to fall down, then the greater trochanter fracture was caused by a direct blow.
J.Orthopaedics 2011;8(1)e17
Keywords: Isolated Ipsilateral lesser and greater trochanteric hip fracture;
Introduction:
There are many hip fractures among elderly patients in Japan: the Japanese Ministry of Health, Labour and Welfare announced that there were 118,000 hip fractures in 2002. Nevertheless, isolated ipsilateral lesser and greater trochanteric hip fractures without intertrochanteric communication in either adults or children have rarely been reported1). We report radiological findings, treatments, and the mechanism of fracture of the present casCase Description: A 92-year-old man was brought to the emergency section of Kasugai Municipal Hospital by ambulance. He lost his balance and fell over when he was apt to ride his bicycle. He could not stand on his right leg. He had dementia, but his family saw what happened, so the details of the injury could be accurately known. His chief complaint was right hip pain. As we had difficulty in his physical examination because of his coxalgia, radiological examination of his right hip was performed. As the type of fracture was uncertain, CT scans and MRI were also carried out.
Radiography of the hip demonstrated avulsion of the lesser trochanter and fracture of the greater trochanter with no apparent intertrochanteric extension (Fig. 1). The fracture condition was well revealed by the CT scan (Fig. 2). MRI showed no typical abnormality at the intertrochanteric lesion (Fig. 3). Laboratory data including full blood cell count were normal. NTX/CR was normal. DEXA scan of vertebral bones showed a bone density 0.925 g/cm2, which is 88% of the means Japanese young adults.
He was made to rest in bed for one week and then gait training was started. He was discharged from the hospital six weeks after admission. One year later, he could walk with one cane.
Discussion:
Hip fractures are common injuries among elderly patients. Among them, nearly all cases were femoral neck fractures or intertrochanteric fractures. Isolated fractures of the greater or lesser trochanter are rare even in elderly patients 2, 3, 5-9). Isolated greater and lesser trochanter fractures without intertrochanteric extension is extremely rare. We could find only one case in the literature: Lower’s report in 1988 1). Its etiology was not clear because the patient had not been able to remember it. It is said that the greater trochanteric fractures are usually caused by a direct blow to the hip 2). Some cases with intertrochanteric extension may be found by MR imaging 3, 4). An isolated avulsion fracture of the lesser trochanter is not common at any age. In young adolescents, isolated lesser trochanter fracture is considered to be an avulsion fracture by iliopsoas muscle traction in active sports, and 85% of cases with this fracture have this etiology 1). In elderly patients, these fractures sometimes occur with no trauma and are often caused by metastatic or primary tumors 5-9).
Figure legends

Fig. 1 Anteroposterior radiograph of right hip on the day of injury
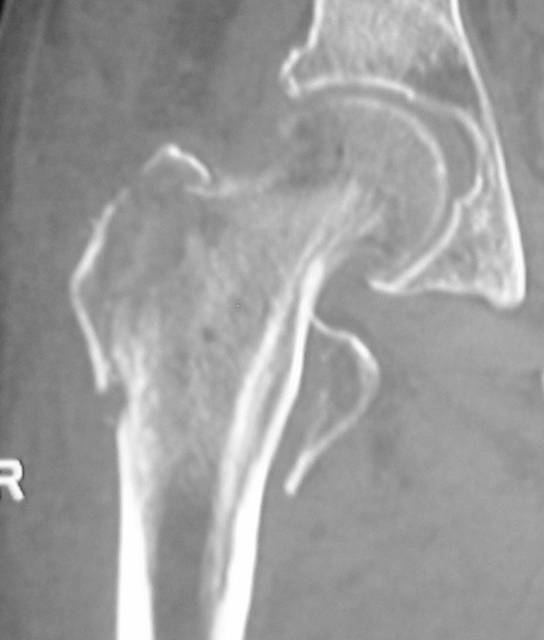
Fig. 2 Reconstructed CT scan of right hip showing isolated fractures of the greater and lesser trochanter
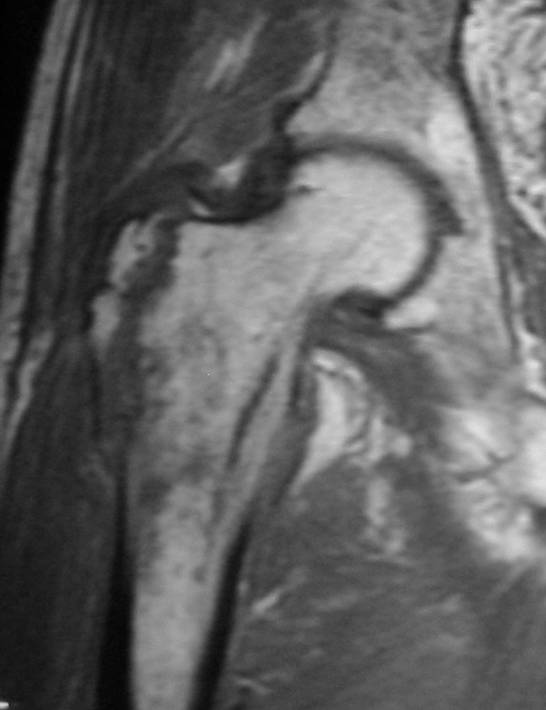
Fig. 3 MRI image showing no intertrochanteric fracture
In our case, there was no apparent metastatic or primary tumor around the proximal femur in CT and MRI. During the follow-up no cancer was found. It is suggested that these fractures happened as follows. First, the lesser trochanter fracture occurred as an avulsion fracture when the patient tried not to fall down, then the greater trochanter fracture occurred by a direct blow. It is considered that conservative therapy should be the first choice for isolated greater and lesser trochanteric fractures. It is said that there exists a risk of misdiagnosis of intertrochanteric fracture around these fractures 3), so MRI and CT scans are very important to avoid to rule out any underlying intertrochanteric lesions.
Conclusion:
Isolated Ipsilateral lesser and greater trochanteric hip fracture is extremely rare. It is suggested that these fractures happened as first, the lesser trochanter fracture occurred as an avulsion fracture when the patient tried not to fall down, then the greater trochanter fracture was caused by a direct blow. MRI and CT scans are very important to avoid misdiagnosis and to rule out any underlying intertrochanteric lesions.
References:
- Lower RF, McNiesh LM, Callaghan JJ, Ipsilateral lesser and greater trochanter fractures of the hip without intertrochanteric extension: a case report. Military Medicine, 1988, 153, 421-423.
- O’rourke MR, Westine SL, Osteonecrosis following isolated avulsion fracture of the greater trochanter in children. J Bone Joint Surg (Am), 2003, 85-A, 2000-2005.
- Craig JG, Moed BR, Eyler WR, Holesbeek M, Fractures of the greater trochanter: intertrochanteric extension shown by MR imaging. Skeletal Radiol, 2000, 29: 572-576.
- Rizzo PF, Gould ES, Lyden JP, Asnis SE, Diagnosis of occult fractures about the hip. J. Bone Joint Surg Am 1993, 75-A: 395-401.
- Dimon JH, III, Isolated fractures of the lesser trochanter of the femur. Clin Orthop, 1972 82: 144-148.
- Bertin KC, Horstman J, Coleman SS, Isolated fracture of the lesser trochanter in adults: an initial manifestation of metastatic malignant disease. J Bone Joint Surg (Am), 1984, 66-A, 770-773.
- Phillips CD, Pope TL, Jr, Jones JE, Keats TE, MacMillan RH III, Nontraumatic avulsion of the lesser trochanter-a pathognomonic sign of metastatic disease? Skeletal Radiol, 1988, 17, 106-110.
- Bonshahi AY, Knowles D, Hodgson SP, Isolated lesser trochanter fractures in elderly-a case for prophylactic DHS fixation. A case series. Injury, Int. J. Care Injured, 2004, 35, 196-198.
- Afra R, Boardman DL, Kabo JM, Eckardt JJ, Avulsion fracture of the lesser trochanter as a result of a primary malignant tumor of bone: J Bone Joint Surg (Am), 1999, 81-A, 1299-1303.
|
|
This is a peer reviewed paper
Please cite as
:Nobuyuki Watanabe:
Isolated Ipsilateral Lesser and Greater Trochanteric Hip Fractures without Intertrochanteric Extension: A Case Report.
J.Orthopaedics 2011;8(1)e17
URL:
http://www.jortho.org/2011/8/1/e17 |
|
|

