|
Abstract:
Spinal fixations with pedicle screws are widely used nowadays in order to provide spine stability and correcting spinal deformity. The pullout strength of pedicle screws can be evaluated by means of pullout strength testing. This paper review recent experimental and finite element analysis evidence concerning the factors that affecting the pullout strength of pedicle screws in various bone materials. Cadaveric bones and synthetic foam blocks were used by researches in the recent experiment. Types of screw, screw designs, insertion technique, bone mineral density and bone-screw interface have their own significant effects to the fixation strength and will be further discussed.
J.Orthopaedics 2011;8(1)e14
Keywords: spinal fixation; pedicle screws; pullout strength; cadaveric bones; synthetic foam blocks
Introduction
Spinal fixation with pedicle screw has become the most commonly used methods in spinal instrumentation system. Their capability in providing fixation stability and the effectiveness in correcting spinal deformity had causes the surgeons to widely used pedicle screws fixation. They have been used also for solid bone fusion in patients with deformity like scoliosis or kyphosis, fracture, spondylolisthesis, degenerative arthritis or tumor [1]. To appraise the stability of the fixation system, a pullout test was done to evaluate the performance of the pedicle screws. In this test, the fixation strength or the holding power of the screw to the bone thread surfaces was determined. Many studies were done by pulling out the embedded screws in either synthetic bone or cadaver bone at a certain rate of withdrawal to determine the pullout strength of particular pedicle screws. However, loosening or failure of pedicle screws were also been reported in many cases. It was due to inadequate of fixation strength of the screw especially in patients with osteoporosis. A lot of efforts have been made in practice to increase the pullout strength of pedicle screw include increasing the length or diameter of the screw, coatings the screw with hydroxyapatite or for severe bone loss, using materials as polymethylmethacrylate (PMMA) and calcium phosphate bone cement [2].
The purpose of the present paper is to summarize recent studies that shows how the pullout performance of various pedicle screws were influenced by several factors including screw designs, cement augmentation, screws coating, pilot hole and tapping, insertional torque and bone density.
Types of Pedicle Screws
Numerous types of pedicle screws were available in market as shown in Figure 1. Many studies were done in order to identify the ability and mechanical performances of each pedicle screw. The holding strength of pedicle screws in vertebral bones was influenced by many factors. The bone-screw interface is the crucial part. There was a report on the capability of conical screws to improve thread purchase by compacting the cancellous bone at the cancellous-cortical interface throughout the pedicle. However, there was a study held to compare conical and cylindrical screws wherein which screws provide better pullout resistances. The holding strength of conical and cylindrical screws was compared under ideal conditions and after a compromising event; cyclic loading and 180° turn back was applied. Cyclic loading was applied because clinical failure of spinal implants is produced most often by fatigue. Pedicle screws are subjected to complex cyclic forces that combine tranverse bending and axial pullout loads. The results showed that conical screws failed more easily when pullout test were performed compared with cylindrical screws for both ideal and compromising event [3]. Conversely, Abshire et al. [4] found inversely results by conducting the same experiments. They declare that conical screws provided an increase in the pullout strength compared with cylindrical screws and no loss of pullout strength, stiffness or energy-to-failure when conical or cylindrical screws were backed out 180° or 360° from full insertion. They also stated that the conical screws engage more of the pedicle cortex as well as the cancellous bone at the corticocancellous margin than cylindrical screws. This contradictory fact is maybe due to the conical and cylindrical screws design that were used in particular studies.
Besides, cortical and cancellous screws were compared in osteoporotic bone material with axial and angled pullout test. The authors found that cancellous screw had a significantly higher pullout force than the cortical screw and they suggest that only screws placed axially or up to 10° angle may increase its holding power. In this study, failure of screw fixation was observed from the stripping of the internal screw threads within the bone material. No failure was observed at the screw treads even after fully pullout of screws. In addition, the bone material itself has a significant effect on the failure of implants. However, limitation was exist in this study wherein the screws diameter used are not identical eventhough the length is equal [5].
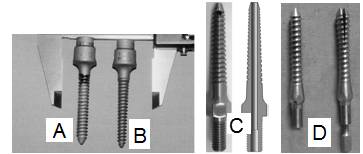
Fig. 1. Several types of typical pedicle screws available: A) cylindrical, B) conical, C) cannulated with radial hole and D) expandable.
A comparative study between cervical pedicle screws and lateral mass screws was done in order to prove that cervical pedicle screws have higher pullout strength using the same screws dimension. Screw loosening has been documented as a failure mechanism for lateral mass screws, where the decreasing size of the lateral masses results in lower pullout strength. In the study, all screws were repetitively cycled at a rate of 25 mm/min for 200 cycles. As hypothesized, pedicle screws have superior pullout strength than the lateral screws. Lateral screws loosen more than the pedicle screws over time, although both screw types have similar initial stability [6]. Thompson et al. [7] have demonstrated that noncannulated screws had better holding power compared with cannulated screws. Cannulated screws are designed with enlarged core diameter to accommodate guide pins. Hence, the ratio of major diameter to core diameter will be decreased and this will affects the pullout strength of cannulated screws. Despite, pullout strength for cannulated pedicle screws could be increased with bone cement augmentation. Chen et al. [8] presented the effects of radial holes for cannulated screws with cement injection on the bone-screw interface. The pullout strength for the cannulated screws increase as the number of radial holes increased. It is because of large amount of exuded cement injection from the radial holes and provides better bone-screw holding strength. They also found that tapping the pilot holes significantly reduced the pullout strength of the screws. A comparison was also made between small-diameter cannulated and solid-core screws by Kissel et al. [9]. They concluded that cannulated and solid core screws of similar dimension and thread length have similar holding strengths. Therefore, these cannulated screws make an attractive alternative for surgical fixation applications.
Various method have been used to improve pedicle screw fixation including increasing the diameter of screws. Yet, this may not always be possible because of anatomic constraints and it may increase the risk for pedicle fracture with possible neural injury. A better solution may be to use an expanding pedicle screws. Expanding pedicle screw may improve bone fixation by increasing the screw tip diameter, allowing for greater bone contact with no increase in pedicle insertion diameter. The screw tip diameter in increased by inserting a smaller gauge screw into the threaded interior of expanding screw and opens the fins concentrically as it advances. Many studies were done to evaluate the pullout performance of expansive pedicle screws. Apparently, expansive pedicle screws had significantly improved pullout strength when compared with self-tapping screws in both cases of low and high bone mineral density (BMD) [10]. Adjunctly, an effort was made by Cook et al. [11] to investigate whether polymethymethacrylate (PMMA) bone cement augmentation of an expandable pedicle screw can further improve fixation strength compared to the expandable screw alone in severely osteoporotic bone. They found that there was an increase in pullout strength with the cemented expandable screw compared with a noncemented expandable screw including a greater than twofold increase in pullout strength in the most severely osteoporotic bone. The stiffness and energy absorbed to failure was also significantly increased. The cement augmentation may be especially useful in the severely osteoporotic patient. Significantly, the removal and replacement of a pedicle screw in a revision procedure substantially decreases the mechanical fixation strength of the screw. Furthermore, the turning back of the screws becomes necessary when surgeons cannot successfully insert screws into the proper position during the first attempt, which reduces the holding strength. Lei et al. [2] have shows that the turning back torque and pullout strength of expansive screws were significantly greater than those conventional screws. Similarly, their pullout strength was higher in the revision test. These findings suggest that expansive screw is ideal in problematic situations where the bone integrity is compromised by either osteoporosis or pedicle screw revision by providing biomechanical parameters similar to those expected for normal bone and in primary surgery.
Pedicle Screw Design
Noteworthy, the designs of pedicle screws are also important in order to provide sufficient fixation strength of the implant. Note that, major diameter, minor diameter, pitch, thread length, thread shape and thread depth of the screws are affecting the pullout strength of the screws (Fig 2). Chapman et al. [12] have conducted a study on factors that affects the pullout strength of cancellous bone screws. In general, cancellous screws are designed to have greater thread depth and decreased thread cross-sectional thickness in comparison to cortical screws, to provide more holding power in porous material such as cancellous bone. Other than that, major diameter of the screw is also give potential effects on the holding power wherein larger diameter provides greater holding power. However, the diameter of screw is limited by the size of pedicles especially the immature pedicles. Yilmaz et al. [1] have done a study to evaluate the effect of dilation of immature pedicles on the pullout strength of the screws. They found that the dilation does not affect the pullout strength of the screws after 3 months in in vivo model. Besides, larger diameter provided a more rigid construct than PMMA augmented pedicle screw fixation in revision spinal instrumentation. The less stiff and more viscoelastic of PMMA would result in reduced stiffness of the construct and increase the ability of distributing creep deformations during fatigue than the large diameter construct [13].

Fig. 2. Parts of typical orthopaedic screw
Studies have been done by numerous researches via finite element analysis. Zhang et al. [14] create a three-dimensional finite element model to simulate the behavior of bone and screw during screw pullout. From the simulation, bone experienced significant shear stress at the thread root during screw pullout. At maximum force, only those elements at the thread root region reached the yield point and failed. They declared that screws with larger major diameter and smaller minor diameter and pitch will lead to an increase in the pullout strength. Moreover, it is obvious that a linear correlation between the pullout strength and thread numbers can be obtained. More thread numbers can resist higher forces or in other words, longer purchase length can effectively increase pullout strength. Chatzistergos et al. [15] were also preferred finite element analysis compared to experimental study. Several factors affecting the pullout forces of screw have been demonstrated. They also found that the major diameter or outer radius is the most important factors and it is proven that larger outer radius yielded greater pullout forces. Without any doubt, they stated that inclination of the thread or thread angle is considered to be the less important ones. However, they did show that an increase of the thread angle resulted in an increase of the pullout force.
Bone Cement Augmentation
Recently, bone cement augmentation was used to enhance the strength of osteoporotic bones and to enhance screw fixation. The technique of bone cement augmentation was crucial aspect since it is reported that the technique is affecting the fixation strength. The techniques for screw fixation with cement augmentation include inserting screws when cement is soft, inserting screws when cement is curing characterized by its doughy consistency and inserting screws after drilling and tapping hardened cement. In the study of Flahiff et al. [16], the fixation strength of polymethymethacrylate (PMMA) bone cement is evaluated among those cement augmentation techniques. They concluded that inserting cortical screws into plastic femur sawbones when the PMMA was in a doughy consistency prior to curing (approximately 8 – 10 min after mixing) produced the strongest cement-screw construct. Drilling and tapping holes after the cement had hardened resulted in the weakest cement-sawbone construct. A biomechanical cadaveric analysis of PMMA augmented pedicle screw fixation was done by Frankel et al. [17]. They highlighted that the screw augmentation procedures were performed using fenestrated bone tap system which can prevent backflow of cement toward neural elements and allowing custom foam for subsequent screw placement. The results showed that PMMA does increase the pullout strength of screw fixation for both osteoporotic and nonosteoporotic bones. In fact, the pullout strength did not significantly change with increased cement volume usage. Thus, they recommended using the lower range of cement volumes in pedicle screw augmentation procedures to perhaps reduce the likelihood of cement toxicity.
Previous method of cement augmentation is the standard transpedicular approach. In addition, other methods of cement augmentation are vertebroplasty augmentation approach and balloon kyphoplasty augmentation as shown in Figure 3. Bone cement is injected through a small hole into a fractured vertebra for vertebroplasty augmentation whilst in kyphoplasty augmentation a balloon is used to create a void which is filled with PMMA. A series of comparison between them has been done by Becker et al. [18] in 2008. Vertebroplasty augmented screws showed a significant higher pullout force than others. Kyphoplasty technique was also increased the pullout force compared with nonaugmented screws. However, surgeons may favor balloon kyphoplasty for screw augmentation

Fig. 3. Cement augmentation method; vertebroplasty (left) and kyphoplasty (right)

Fig. 4. a) Coated and b) uncoated screws (left) and PMMA augmented screw (right)
since vertebroplasty has considerable risks regarding cement leakage and a slightly higher perioperative morbidity. By the study of Burval et al. [19], they evaluate the performance of kyphoplasty augmentation with an exposed to cyclic fatigue loading prior to pullout testing. 5000 cycles of caudalcephalad loading were applied perpendicular to the pedicle screws. Their results showed that pedicle screw augmentation using kyphoplasty technique increased the pullout failure 2-3 fold in osteoporotic vertebrae. Chang et al. [20] agreed that PMMA has advantages like readily availability, inexpensiveness, short application time and fixation strength that are practical for clinical applications. Sequential dilatation with K-wires during screw tract preparation can be used to prevent leakage of PMMA cement. They also declared that the sufficient usage volumes of PMMA cement for lumbar and thoracic screw are 3 mL and 2 mL respectively. As hypothesized by Blattert et al. [21], removal of screws, if needed, might cause problems. Among screw designs, the cannulated-fenestrated screws might cause problems especially during revision, because of their winglike cement interconnection between the screw core and surrounding tissue. However, they have successful showed that revision characteristics of these screws following cement augmentation are not problematic even for osteoporosis cases. Obviously, the cement interconnection between the screw core and surrounding bone tissue is fragile enough to break off in the event of extraction torque and to release the screw.
Other types of bone cements instead of PMMA are calcium sulfate paste and particulate calcium phosphate. Rohmiller et al. [22] suggested that PMMA should be replaced by calcium sulfate paste since they demonstrated similar pullout strength. PMMA has potential dangers if leakage into spinal canal were occurred. In addition, the calcium sulfate paste doesn’t have an exothermic reaction in its curing phase and this will eliminates the risk of thermal damage to spinal canal. The paste also improves safety around spinal cord since it is biodegradable and designed to be resorbed by body rather than becoming a permanent space-occupying lesion in the canal in the event of leakage. Particulate calcium phosphate is alternative bone cement to PMMA. The special ability of the calcium phosphate in the fixation application is to speed natural tissue healing and then be replaced by the patient’s own bone tissue. It has been demonstrated that the pullout strength of screws with augmentation of calcium phosphate is high. Interestingly, the application of calcium phosphate to normal bone will reduce screw pullout strength. Calcium phosphate improved the pullout strength of failed screw in low density polyurethane blocks (osteoporotic bone) [23].
Pedicle Screws Surface Coating
As described early, PMMA may be associated with complication such as leakage, exothermic damage to the bone and adjacent tissue and long term screw loosening resulting from nonbiologic bonding. The use of hydroxyapatite (HA) coated implants (Figure 4), on the other hand, may improve the stability of the bone-metal interface without the disadvantages of PMMA [24, 25]. Hasegawa et al. [26] have showed that HA-coated pedicle screws have higher pullout resistance than uncoated screws and it is clearly revealed that the inter-spaces between the screw threads had filled with new bone and good bonding was present between the bone and the apatite coating of the screw. Even under loaded conditions, HA coating improves fixation of pedicle screws, with increased pullout resistance and reduced risk of loosening. As stated by Sanden et al. [27], higher pullout resistance by HA-coated screws at early stage was mainly caused by differences in surface roughness of the coatings while the difference at later stage was doe to bone reaction around the HA-coated screws. A study on improving extraction torque of HA-coated pedicle screws was also been done. The surface roughness of plasma-sprayed HA-coated implants is generally three to four times greater than the roughness of machined metal implants [28]. The fixation strength of HA-coated screws was highly correlated to its surface roughness. By using fully coated screws, extraction was extremely difficult compared to extraction of conventional stainless steel screws, which were regularly loose. By reducing the area of the screws that is coated, it may be possible to achieve an enhanced purchase while extraction will be easier [29]. Titanium coated on the surface of titanium alloy implants have also been widely used in orthopaedics and dentistry with great success because of their good mechanical properties and biocompability rather than HA coatings. However, titanium coating is bioinert, which cannot bond chemically to bone tissue. Therefore, attempts have been made including modification of titanium coating with alkali and heat treatment to improve the surface properties of titanium coating implants [30]. Absolutely, alkali-modified implants shows higher shear strength which can be attributed to the changes in surface topography and chemistry. Significantly, it can improve and accelerate the early ingrowth of bone and osseointegration to reduce clinical healing times and thus to improve implant success rates [31]. Upasani et al. [32] had pointed the benefits of hydroxyapatite – titanium plasma sprayed (HA-TPS) composite coating that may leverage the advantages of both individual coatings to further improve screw fixation. Generally, HA-TPS did improved peak torque during screw extraction. However, the composite coating may not provide a significantly greater benefit compared with HA alone. They clarified that improved osseointegration with HA coatings may result in a decreased incidence of screw loosening and improved outcomes of transpedicular spinal instrumentation in nonfusion procedures.
Other Factors Influencing Fixation Strength
Few reports have addressed the effects of pilot hole tapping on the bone/screw interfacial strength. However, the reported results have been inconsistent. Thompson et al. [7] examined the effect of tapping on pullout strength in synthetic polyurethane foam. Their results indicated there was no demonstrable effect on holding power when screws were inserted with or without tapping. Chapman et al. [12] indicated that tapping in porous materials decreased screw pullout strength because the removal of materials by the tap enlarged the hole considerably, reducing the holding power of the screw threads. Ronderos et al. [33] analyzed the axial pullout strength of tapped vesus untapped pilot holes for bicortical screws in the anterior cervical spine. They concluded that tapping a pilot hole neither weakens nor strengthens the axial pullout strength of fully threaded cortical bone screws. Carmouche et al. [34] found that tapping the pedicles in the lumbar spine did decrease the pullout resistance but not in thoracic spine. One explanation for this is that in severe osteoporosis, there is simply less cancellous bone available to be compressed. Thus, the process of tapping does not cause a significant net loss of cancellous bone and fixation is more dependent on cortical purchase.
A pilot hole is drilled with smaller diameter to make a path so that screws can easily be inserted in correct direction. Pilot hole was also said that it has its own affects on pullout resistance and insertion torque. Leite et al. [35] found that higher insertion torque can be resulted as long as the pilot hole used was smaller than inner or minor diameter of screw. In other words, with the increased diameter of the pilot hole, the insertion torque was reduced. That phenomenon would be correlated with bone removal during pilot hole drilling which would affect the anchorage of the implant. As the pilot hole’s diameter increases, a larger amount of bone is removed, and a smaller amount of bone is available to be compacted around the implant, thus, reducing the insertion torque. During the surgical procedure, insertion, removal and re-insertion of the screws are often happen to determine the pathway of pilot hole and to detect possible violations of the lateral wall of the pilot hole that might damage adjacent structures of vertebrae [36]. However, this procedure might interfere with the screw holding strength. Therefore, Defino et al [37] investigate the effect of repetitive pilot hole use on the insertion torque and pullout strength of screws. They found that insertion torque and pullout strength did reduce between the first and following insertion. Despite, the pattern of reduction of pullout strength was not similar to the pattern of reduction of the insertion torque. However, the study of Foley et al. [38] revealed that there was no significant difference in pullout strength was noted in pretapped or self-tapped screws inserted into the same hole one, two or three times before pullout testing.
Besides, the effect of insertional torque to pullout resistance is uncertain. Leite et al. [35] stated that the insertion torque of implants showed a correlation with pullout resistance only for perforation values of pilot hole smaller than the inner diameter of the screw. Inceoglu et al. [39] found that there was no significant correlation between pullout strength and insertional torque. They concluded that insertional torques are not good predictors of pullout strength and stiffness, particularly in nonstandard screw and thread designs.
Bone mineral density (BMD) is another factor that influenced pullout strength especially in osteoporosis cases. Many studies have shown the correlation between BMD and pullout strength. Hsu et al. [40] agreed that both pullout strength and insertion torque in the foam with the higher density was consistently higher than that in the foam with the lower density. Battula et al. [41] concluded that the depth of insertion of the tip of the screw for adequate fracture fixation in normal bone is 1 mm or more past the far cortex and in osteoporotic bone it is at least 2 mm past the far cortex. It shows that osteoporotic bone need more screws surface area interface with the bone in order to provide sufficient holding power. Osteoporotic bones usually related to screw loosening that mainly caused by cyclic caudocephalad toggling at the bone-screw interface when an axial compression load was transmitted through the plate or rod to the screw. A clinical study was done by Okuyama et al. [42] to see the screw loosening behavior among osteoporosis patients. After several years followed up, loosening of pedicle screws occurred and it affect the implant stability. Thus, BMD is supposed to be a very important parameter influencing the stability of pedicle screws. Suzuki et al. [43] found that pedicle screw coupling increased the pullout strength in osteoporotic spine. However, the improvement is only subjected to BMD of more than 90 mg/ml but not for BMD of less than 90 mg/ml. Zhang et al. [44] noted that screw pullout strengths were directly proportional to the shear strength of the foam material. Low BMD will have lower pullout strength as their shear strength is very low. Ramaswamy et al. [45] studied the holding power of screws in osteoporotic, osteopenic and normal bone. They found that the pullout strengths of all screws were correlated to the foam density and significantly it was better in higher density foam.
Conclusion
The main factors affecting the pullout force of a bone screw are its design, the material properties of the bone and the insertion technique followed by the surgeon. Conflicts are still exist whether to perform experimental study using cadaver or synthetic foam blocks since results may vary within the materials. A continuous study must keep on doing to gather information and knowledge as much as possible to enhance more stable and rigid spinal fixation system. Extra concern must be put on to the osteoporosis cases since major problems of fixation stability and rigidity are referring to them.
References:
1-G. Yilmaz, G. Demirkiran, C. Ozkan, K. Daglioglu, V. M. Pekmezci, A. Alanay and M. Yazici (2009), The effect of dilation of immature pedicles on pullout strength of the screws, Spine 34, 2378 – 2383
2-W. Lei and Z. Wu (2006), Biomechanical evaluation of an expansive pedicle screw in calf vertebrae, European Spine 15, 321 – 326.
3-C. A. Lill, U. Schlegel, D. Wahl and E. Schneider (2000), Comparison of the in vitro holding strengths of conical and cylindrical pedicle screws in a fully inserted setting and backed out 180°, Spinal Disorders 13, 259 – 266.
4-B. B. Abshire, R. F. McLain, A. Valdevit and H. E. Kambic (2001), Characteristics of pullout failure in conical and cylindrical pedicle screws after full insertion and back-out, Spine 1, 408 – 414.
5-P. S. D. Patel, D. E. T. Shepherd and D. W. L. Hukins (2008), Axial and angled pullout strength of bone screws in normal and osteoporotic bone material, ICBME Proceedings 23, 1619 – 1622.
6-T. L. Johnson, E. E. Karaikovic, E. P. Lautenschlager and D. Marcu (2006), Cervical pedicle screws vs. lateral mass screws: uniplanar fatigue analysis and residual pullout strengths, Spine 6, 667 – 672
7-J. D Thompson, J. B. Benjamin and J. A. Szivek (1997), Pullout strengths of cannulated and noncannulated cancellous bone screws, Clinical Orthopaedics and Related Research 341, 241 – 249.
8-L. H. Chen, C. L. Tai, P. L. Lai, D. M. Lee, T. T. Tsai, T. S. Fu, C. C. Niu and W. J. Chen (2009), Pullout strength for cannulated pedicle screws with bone cement augmentation in severely osteoporotic bone: Influences of radial hole and pilot hole tapping, Clinical Biomechanics.
9-C. G. Kissel, S. C. Friedersdorf, D. S. Foltz and T. Snoeyink (2003), Comparison of pullout strength of small-diameter cannulated and solid-core screws, Foot and Ankle Surgery, 334 – 338.
10-S. D. Cook, S. L. Salkeld, T. S. Whitecloud III and J. Barbera (2000), Biomechanical evaluation and preliminary clinical experience with an expansive pedicle screw design, Spinal Disorders 13, 230 – 236
11-S. D. Cook, S. L. Salkeld, T. Stanley, A. Faciane, S. D. Miller (2004), Biomechanical study of pedicle screw fixation in severely osteoporotic bone, Spine 4, 402 – 408.
12-J. R. Chapman, R. M. Harrington, K. M. Lee, P. A. Anderson, A. F. Tencer and D. Kowalski (1996), Factors affecting the pullout strength of cancellous bone screws, Biomechanical Engineering 118, 391 – 398.
13-D. W. Kiner, C. D. Wybo, W. Sterba, Y. N. Yeni, S. W. Bartol and R. Vaidya (2008), Biomechanical analysis of different techniques in revision spinal instrumentation: Larger diameter screws versus cement augmentation, Spine 33, 2618 – 2622.
14-Q.H. Zhang, S.H. Tan, S.M. Chou (2004), Investigation of fixation screw pull-out strength on human spine, Biomechanics 37, 479-485.
15-P. E. Chatzistergos, E. A. Magnissalis and S. K Kourkoulis (2009), A parametric study of cylindrical pedicle screw design implications on the pullout performance using an experimentally validated finite-element model, Medical Engineering and Physics.
16-C. M. Flahiff, G. A. Gober and R. W. Nicholas (1995), Pullout strength of fixation screws from polymethylmethacrylate bone cement, Biomaterials 16, 533 – 536.
17-B. M. Frankel, S. D’ Agostino and C. Wang (2007), A biomechanical cadaveric analysis of polymethylmethacrylate-augmented pedicle screw fixation, Neurosurgical Spine 7, 47 – 53.
18-S. Becker, A. Chavanne, K. Kropik, N. Aigner, M. Ogon and H. Redl (2008), Assessment of different screw augmentation techniques and screw designs in osteoporotic spines, Eur Spine, 1462 – 1469.
19-D. J. Burval, R. F. McLain, R. Milks and S. Inceoglu (2007), Primary pedicle screw augmentation in osteoporotic lumbar vertebrae, Spine 32, 1077 – 1083.
20-M. C. Chang, C. L. Liu and T. H. Chen (2008), Polymethylmethacrylate augmentation of pedicle screw for osteoporotic spinal surgery, Spine 33, 317 – 324.
21-T. R. Blattert, S. Glasmacher, H. J. Riesner and C. Josten (2009), Revision characteristics of cement-augmented, cannulated-fenestrated pedicle screws in the osteoporotic vertebral body: A biomechanical in vitro investigation, Neurosurgery Spine 11, 23 – 27.
22-M. T. Rohmiller, D. Schwalm, R. C. Glattes, T. G. Elalayli and D. M. Spengler (2002), Evaluation of calcium sulfate paste for augmentation of lumbar pedicle screw pullout strength, Spine 2, 255 – 260.
23-A. Hashemi, D. Bednar and S. Ziada (2009), Pullout strength of pedicle screws augmented with particulate calcium phosphate: An experimental study, Spine 9, 404 – 410.
24-S. Stea, M. Visentin and L. Savarino (1995), Microhardness of bone at the interface with ceramic-coated metal implants, Biomedical Materials Research 29, 695–699.
25-A. Moroni, S. Toksvig-Larsen and M.C. Maltarello (1998), Comparison of hydroxyapatite-coated, titanium-coated, and uncoated tapered external-fixation pins, Bone and Joint Surgery 80A, 547–554.
26-T. Hasegawa, A. Inufusa, Y. Imai, Y. Mikawa, T. H. Lim and H. S. An (2005), Hydroxyapatite-coating of pedicle screws improves resistance against pullout force in the osteoporotic canine lumbar spine model: A pilot study, Spine 5, 239 – 243.
27-B. Sanden, C. Olerud, and S. Larsson (2001), Hydroxyapatite coating enhances fixation of loaded pedicle screws: A mechanical in vivo study in sheep, Eur Spine 10, 334 – 339.
28-A. Wennerberg, T. Albrektsson and B. Andersson (1993), Design and surface characteristics of 13 commercially available oral implants systems, Oral Maxillofac Implants 8, 622 – 633
29-B. Sanden, C. Olerud, C. Johansson and S. Larsson (2000), Improved extraction torque of hydroxyapatite-coated pedicle screws, Eur Spine 9, 534 – 537.
30-T. Kokubo, F. Miyaji, H. M. Kim and T. Nakamura (1996), Spontaneous formation of bonelike apatite layer on chemically treated titanium metals, American Ceramic Society 79, 1127 – 1129.
31-W. Xue, X. Liu, X. B. Zheng and C. Ding (2005), In vivo evaluation of plasma-sprayed titanium coating after alkali modification, Biomaterials 26, 3029 – 3037.
32-V. V. Upasani, C. L. Fransworth, T. Tomlinson, R. C. Chambers, S. Tsutsui, M. A. Slivka, A. T. Mahar and P. O. Newton (2009), Pedicle screw surface coatings improve fixation in nonfusion spinal construct, Spine 34, 335 – 343.
33-J. F. Ronderos, R. Jacobowitz, V. K. H. Sonntag,N .R. Crawford and C. A. Dickman (1997), Comparative pull-out strength of tapped and untapped pilot holes for bicortical anterior cervical screws, Spine 22, 167 – 170.
34J. J. Carmouche, R. W. Molinari, T. Gerlinger, J. Devine and T. Patience (2005), Effects of pilot hole preparation technique on pedicle screw fixation in different regions of the osteoporotic thoracic and lumbar spine, Neurosurg Spine 3, 364 – 370.
35-V. C. Leite, A. C. Shimano, G. A. P. Goncalves, F. Kandziora and H. L. A. Defino (2008), The influence of insertion torque on pedicular screw’s pullout resistance, Acta Ortop Bras 16, 214 – 216
36-Y. J. Kim and L. G. Lenke (2005), Thoracic pedicle screw placement: free hand technique, Neurol India 53, 512 – 519.
37-H. L. A. Defino, R. C. Rosa, A. C. Shimano, J. B. Volpon, F. J. A. Paula, P. Schleicher, K. Schnake and F. Kandziora (2009), The effect of repetitive pilot-hole use on the insertion torque and pullout strength of vertebral system screws, Spine 34, 871 – 876.
38-W. L. Foley, D. E. Frost and M. R. Tucker (1990), The effect of repetitive screw hole use on the retentive strength of pretapped and self-tapped screws, Oral Maxillofac Surgery 48, 264 – 267
39-S. Inceoglu, L. Ferrara and R. F. McLain (2004), Pedicle screw fixation strength: pullout versus insertional torque, Spine 4, 513 – 518.
40-C. C. Hsu, C. K. Chao, J. L. Wang, S. M. Hou, Y. T. Tsai and J. Lin (2005), Increase of pullout strength of spinal pedicle screws with conical core: biomechanical tests and finite element analyses, Orthopaedic Research 23, 788 – 794.
41-S. Battula, A. Schoenfeld, A. Vrabec and G. O. Njus (2006), Experimental evaluation of the holding power/stiffness of the self-tapping bone screws in normal and osteoporotic bone material, Biomechanics 21, 533 – 537.
of the holding power/stiffness of the self-tapping bone screws in normal and osteoporotic bone material, Biomechanics 21, 533 – 537
42-K. Okuyama, E. Abe, T. Suzuki, Y. Tamura, M. Chiba and K. Sato (2001), Influence of bone mineral density on pedicle screw fixation: A study of pedicle screw fixation augmenting posterior lumbar interbody fusion in elderly patients, Spine 1, 402 – 407
43-T. Suzuki, E. Abe, K. Okuyama and K. Sato (2001), Improving the pullout strength of pedicle screws by screw coupling, Spinal Disorders 14, 399 – 403
44-Q. H. Zhang, S. H. Tan and S. M. Chou (2006), Effects of bone materials on the screw pull-out strength in human spine, Medical Engineering & Physics 28, 795 – 801
45-R. Ramaswamy, S. Evans and Y. Kosahvili (2009), Holding power of variable pitch screws in osteoporotic, osteopenic and normal bone: Are all screws created equal?, Injury .
|

