|
J.Orthopaedics 2007;4(4)e12
index.htm
Introduction:
Simultaneous bilateral elbow dislocation is rare injury and only
13 cases are reported in literature. 9 cases were purely
ligamentous injury and 4 cases were associated with additional
osseous injury. Untreated or neglected unilateral dislocation of
elbow is not uncommon in developing countries but untreated or
neglected simultaneous bilateral elbow dislocation has not been
reported in English literature.
We report an unusual case of simultaneous bilateral elbow
dislocation of elbow which was untreated for 9 months making her
handicap for daily activities of living.
Material and Methods :
After 9 months of fall injury from tree about 10mts height, a 30
years old female presented in Dhulikhel Hospital complaing of
inability to flex both elbow sufficiently to feed herself and to
take care of personal hygiene like washing face or combing hair
or buttoning clothes and applying bindis over forehead. She
was dependent to her children for these activities. Otherwise
she had to take food or drink like canines by bringing mouth to
the plate. Clinical examinations and radiographic investigations
revealed bilateral posterior dislocation of elbow with mature
myositis mass on right side and ununitted olecranon fracture on
left side with intact distal neurovascular structures on both
sides. Range of movement of right and left elbow was 4-10˚ and
8-22˚ respectively with restricted pronation on both sides (Fig:
1a)

Figure 1a: Range of movement of elbow before surgery.
Figure 1b, 1c: Pre operative and post operative radiographs.
Open reduction and radio humeral Kirschner wire fixation was
done of both elbow in a week apart as described by Speed JS for
old unreduced elbow dislocation.1 Myositis mass was
excised on right elbow and tension band wiring for fracture
olecranon was done on left elbow (Fig: 1b,c). Ulnar
nerve was transposed anteriorly on both sides. On 5th
post operative day, oozing of fresh blood was noted from
incision site of right elbow and on removal of clots; there was
continuous trickling of fresh blood. Distal radial pulsation was
intact. Coagulation profiles were within normal range. Colour
flow arterial doppler ultrasonography revealed pseudo-aneurysm
of brachial artery about 2.5cm proximal to bifurcation into
cubital fossa (Fig: 2). Brachial artery was explored; distal and
proximal mobilization was done; pseudo-aneurysmal sac was
excised and end to end anastomosis was performed (Fig: 3). Post
operative events were uneventful. Active movement of left elbow
was started on 2nd postoperative week after removal
of radio humeral Kirschner wire but delayed incremental range of
movement was started on right side.

Figure 2: Doppler ultrasonography showing brachial artery
(BA) and aneurysmal sac (AS).
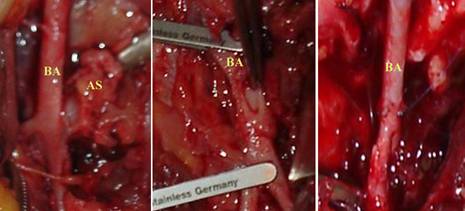
Figure 3: Exploration of brachial artery (BA) and
aneurysmal sac (AS): before and after end to end anastomosis
During last follow up period after 1 year of surgery, range of
movement of right and left elbows was 15-100˚ and 0-90˚
respectively with full supination and terminally restricted
pronation (Fig: 4). Distal neuro- vascular structures were
intact and she was no longer dependent over her children for her
previous disabilities.

Figure 4: Range of movement of both elbows at 12 months follow up.
Discussion:
Though the elbow is highly constrained and stable joint,
dislocation is common injury especially in 10 -20 yrs of
population .2 Posterior elbow dislocation occurs when
valgus and external ratatory torque is applied when a person
fall with elbow in extension or in flexion .3
Unreduced posterior dislocation which is primarily seen in
developing countries is one of the challenges for restoring
stable and functional range of movement in the presence of
incipient or established soft tissue contracture. Unilateral
untreated dislocation may be compatible with life with
difficulties but when it is bilateral as in our case, patients
routine activities are severely affected because of restriction
of bilateral elbow movement. Socio- economic factors are major
constraints that prevent patients seeking for medical help
despite severe disabilities. English literature search revealed
only cases of simultaneous bilateral neglected dislocation of
elbow which had been promptly relocated.
Kovrizhnyi VG et al, Maitra AK and Schonbauer HR had reported
bilateral simultaneous dislocation of elbow in literature. 4, 5,
6 Syed AA et al. reported a case of simultaneous bilateral elbow
dislocation with unilateral radial head fracture in a female
gymnast which was promptly reduced followed by immediate
mobilization .7 Koslowsky TC et al. had found two cases of
simultaneous bilateral elbow dislocation following fall from 5
mts. tall ladder and mountain bike respectively. Three elbows
were reduced with closed technique and one with open method. All
elbows were actively mobilized with external fixator with motion
capacity and resulted into excellent clinical outcomes.8
Injury to brachial artery with closed elbow dislocation without
osseous injury is also rare (5-13%).9 Injuries to part of the
vessel wall without complete rupture or transsection can give
rise to pseudo-aneurysm which is a late sequalae of trauma and
may not be detected early because it may not disturb distal
pulsation. Pseudo-aneurysm of size less than 2 cm may be silent,
asymptomatic and may go unnoticed for long time during long
enlarging period unless it compresses surrounding nerves or
causes thrombo- embolic phenomena to distal part or produces
pulsatile mass.10 In our case pseudo-aneurysm sac probably got
injured during surgery and detected when it started leaking post
operatively.
When pseudo aneurysm is detected, treatments are surgical
reconstruction or color-doppler ultrasonographic guidance
ligation, endovascular graft implantation, embolization or
ultrasound-guided thrombin injection. A single small aneurysm
distal to the brachial bifurcation can be ligated but aneurysm
at the brachial truncus or in the distal region, reconstruction
is necessary for the viability of the extremity, as in our
patient.10
Old unreduced simultaneous bilateral dislocation of elbow with
severe disabilities is still found in developing country like
Nepal. Open reduction, V-Y plasty of triceps muscle and early
mobilization of elbow with can add good range of movement. In
cases with neglected dislocation of elbow, traumatic
pseudo-aneurysm of distal part of brachial artery should be
ruled out before surgery.
Reference :
1.
Speed JS. An operation for unreduced posterior
dislocation of the elbow. South Med J; 1925, p18:193.
2.
Hotchkiss RN. Fracture and dislocations of elbow. In:
Rockwood CA, Green DP, Bucholz RW, Heckman JD (eds)
Fracture in Adult. 4th ed. Vol. 1. Lippincott
Raven, Philadelphia; 1996, p 929-1024.
3.
Kovrizhnyi VG, Savvin EM. A case of simultaneous
bilateral luxation in the elbow joint. Klin Khir; 1969,
5: p65.
4.
Sojbjerg JO, Helmig P, Kjaersgaard AP. Dislocation of
the elbow: an experimental study of the ligamentous injuries.
Orthopedics; 1989, 12(3): p461- 3.
5.
Maitra AK. A rare case of bilateral simultaneous
posterior dislocation of the elbow. Br J Clin Pract;
1979, 33(8): p233-5.
6.
Schonbauer HR. Simultaneous, bilateral dislocation of
the elbow. Monatsschr Unfallheilkd Versicherungsmed;
1957, 60(4): p119-21.
7.
Syed AA, O'Flanagan J. Simultaneous bilateral elbow
dislocation in an international gymnast. Br J Sports Med;
1999, 33(2):p132-3.
8.
Koslowsky TC, Mader K, Siedek M, Pennig D. Treatment of
bilateral elbow dislocation using external fixation with
motion capacity: a report of 2 cases. J Orthop Trauma;
2006, 20(7): p499-502.
9.
Platz A, Heinzelmann M, Ertel W, Trentz O. Posterior
elbow dislocation with associated vascular injury after blunt
trauma. J Trauma; 1999, 46(5): p948-50.
10.
Yetkin U, Gurbuz A. Post-Traumatic Pseudoaneurysm of
the Brachial Artery and Its Surgical Treatment. Tex Heart
Inst J; 2003, 30(4): p 293297.
|

