|
Abstract
Solitary metastatic renal cell carcinoma to
the radius is uncommon. We present such a case treated with
surgery and reconstruction with non-vascularised fibula graft.
Postoperatively there was progression of the disease with
involvement of the proximal radius. Eventually the disease was
controlled with adjuvant treatment.
Key words: metastatic lesion; renal cell carcinoma
J.Orthopaedics 2006;3(3)e7
Introduction:
Bone metastases of renal
cell carcinoma is believed to be somewhere near 50 per cent (6).
The metastatic deposits are rather multiple than solitary ones.
Reconstruction after excision of the distal radius with non-vascularised
fibula graft is one of the current methods of treatment. It is
anticipated that clear surgical margins are achieved to prevent
recurrence of the disease. In our case, despite the clear bone
margins achieved with surgery and reconstruction with
non-vascularised fibula graft, there was an
unusual progressive metastatic disease in the proximal radius.
Case Report
 A
45 year old, right hand dominant male presented to our
department with a six-week history of right wrist pain.
Examination revealed a diffuse swelling and tenderness over the
right distal radius, without infiltration of the skin and no
distal neurovascular deficit. No regional lymph nodes were
palpable. Wrist movements were limited by pain. An X-ray showed
an aggressive lytic lesion involving the distal radial
metaphysis and styloid process. A subsequent whole bone
scintigraphy and CT A
45 year old, right hand dominant male presented to our
department with a six-week history of right wrist pain.
Examination revealed a diffuse swelling and tenderness over the
right distal radius, without infiltration of the skin and no
distal neurovascular deficit. No regional lymph nodes were
palpable. Wrist movements were limited by pain. An X-ray showed
an aggressive lytic lesion involving the distal radial
metaphysis and styloid process. A subsequent whole bone
scintigraphy and CT
 scan
of the chest did not reveal any other lesions. A CT scan of the
abdomen and pelvis revealed a left renal mass suggestive of
renal carcinoma. MRI of the forearm showed a large expansile
lesion of the distal radius (fig 1). A biopsy of the lesion
confirmed a metastatic renal cell carcinoma. He underwent
excision of the right distal radius and reconstruction with non-vascularised
proximal right fibula graft (fig 2). scan
of the chest did not reveal any other lesions. A CT scan of the
abdomen and pelvis revealed a left renal mass suggestive of
renal carcinoma. MRI of the forearm showed a large expansile
lesion of the distal radius (fig 1). A biopsy of the lesion
confirmed a metastatic renal cell carcinoma. He underwent
excision of the right distal radius and reconstruction with non-vascularised
proximal right fibula graft (fig 2).
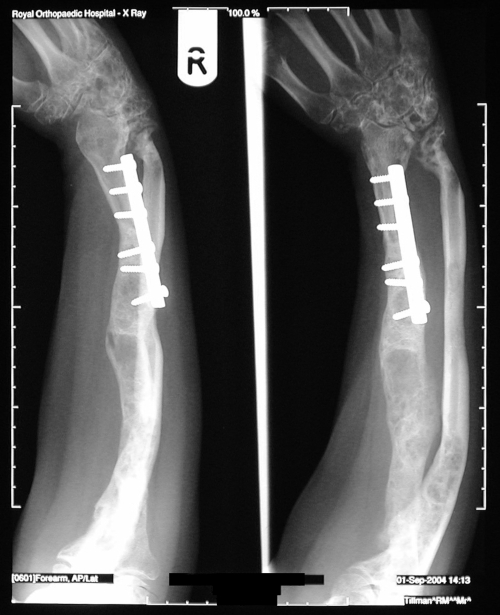
 The
incision was planned in order to incorporate the biopsy tract.
The tumour-bearing portion of the radius along with healthy bone
margins was excised en bloc. The proximal fibula from the
ipsilateral leg was used to replace the excised radius and fixed
with six hole DC plate with compression. The renewed radial
carpal and radial ulna joints were stabilised with Kirscher
wires. An above-the-elbow plaster cast was applied which was
retained for 6 weeks. It was then replaced by an above-the-elbow
removable cast after removal of the Kirscher wires.Histology of
the excised specimen confirmed clear cell carcinoma with clear
bone resection margins. The
incision was planned in order to incorporate the biopsy tract.
The tumour-bearing portion of the radius along with healthy bone
margins was excised en bloc. The proximal fibula from the
ipsilateral leg was used to replace the excised radius and fixed
with six hole DC plate with compression. The renewed radial
carpal and radial ulna joints were stabilised with Kirscher
wires. An above-the-elbow plaster cast was applied which was
retained for 6 weeks. It was then replaced by an above-the-elbow
removable cast after removal of the Kirscher wires.Histology of
the excised specimen confirmed clear cell carcinoma with clear
bone resection margins.
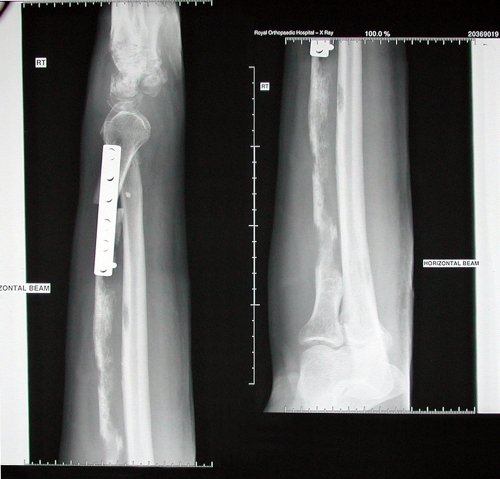 An
X-ray of his right forearm taken six weeks postoperatively
showed rapid progression of metastasis in the whole radius with
extensive destruction of the remnant radius and multiple
destructive foci in the ulna and wrist joint (fig 3a,b).
Following that he had a nephrectomy and was then referred to the
oncologists who offered him palliative radiotherapy and
interferon alpha treatment (IFN-a). He received irradiation,
35Gy in ten fractions to his right forearm, and started on IFN-a
treatment, 10 mega units three times a week. About a year after
initial presentation he was reviewed in the outpatient
department. An X-ray taken then, showed that there was
regeneration of the radius and ulna bones. An
X-ray of his right forearm taken six weeks postoperatively
showed rapid progression of metastasis in the whole radius with
extensive destruction of the remnant radius and multiple
destructive foci in the ulna and wrist joint (fig 3a,b).
Following that he had a nephrectomy and was then referred to the
oncologists who offered him palliative radiotherapy and
interferon alpha treatment (IFN-a). He received irradiation,
35Gy in ten fractions to his right forearm, and started on IFN-a
treatment, 10 mega units three times a week. About a year after
initial presentation he was reviewed in the outpatient
department. An X-ray taken then, showed that there was
regeneration of the radius and ulna bones.
 He
was pain free; he had a fixed deformity of 45 degrees at the
elbow with deformed and curved forearm with no movement at the
wrist, no rotation of the forearm and stiff MCP joints. He
was pain free; he had a fixed deformity of 45 degrees at the
elbow with deformed and curved forearm with no movement at the
wrist, no rotation of the forearm and stiff MCP joints.
He was still being treated
with interferon and a year later he was reviewed in the clinic
again. He was pain free and examination of his right upper limb
showed loss of extension at the elbow with elbow flexion from 70
degrees to 130 degrees of flexion. His wrist joint and finger
joints were very stiff but improving with physiotherapy. X-rays
of his radius and ulna showed remarkable consolidation of the
radius, which had previously been almost completely destroyed by
the tumour (fig 4). The graft had healed fully.
Discussion :
The fact that renal cell
carcinoma (RCC) metastasises to the skeleton is well known. The
metastatic deposits are generally multiple, and only
occasionally solitary, and they generally involve the axial
skeleton or the proximal parts of the long bones (particularly
the femur and humerus) or both (1). Metastatic renal cell
carcinoma remains a disease that is highly resistant to systemic
therapy and difficult to treat. In the last few years,
randomised studies have demonstrated a survival advantage for
patients receiving immunotherapies such as Interferon alpha (IFN-a)
although this advantage is marginal (5).
The use of autografts in
reconstruction of skeletal defects following tumour surgery has
been well documented (3). Al-Zahrani et al (2) and Mack et al
(5) have showed that the non-vascularised single fibular graft
is still valid to bridge bone defects.Aggarwal et al (1)
reported a case of solitary metastasis to the radius of renal
cell carcinoma treated successfully with excision and fibula
bone grafting only. There was no recurrence of the disease in
that case.To our knowledge this unusual behaviour of a
metastatic renal cell carcinoma of distal radius treated with
surgery and autologous non-vascularised fibula graft has not
been reported in the medical literature.
The case we report here is
of interest in that: (a) it was a solitary metastasis, (b) it
involved the distal radius, (c) there was progression of the
disease after treatment by excision and reconstruction with non-vascularised
fibula graft. Recurrence of the metastatic renal cell carcinoma
at the fibula graft site and progression of the disease to the
proximal radius despite clear bone margins was very unusual. In
our patient, surgery alone failed to control the disease, which
responded though very well to adjuvant radiotherapy and
immunotherapy with IFN-a.
Reference :
-
Aggarwal ND, Mittal RL,
Bhalla R. Delayed solitary metastasis to the radius of renal
cell carcinoma. J Bone Joint Surg 1972 ; 54(6)-A : 1314-1316.
-
Al-Zahrani S, Harding
MGB, Khan FA, Ikram A, Takroni T. Free fibular graft still has
a place in the treatment of bone defects. Injury 1993; 24(8) :
551-554.
-
Enneking WF, Eady JL,
Burchardt H. Autogenous cortical bone grafts in the
reconstruction of segmental skeletal defects. J Bone Joint
Surg 1980; 62-A : 1039.
-
Mack GR, Lichtman DM,
MacDonald RI. Fibular autografts for distal defects of the
radius. J Hand Surg 1979; 4 : 576-583.
-
Nanus DM. New treatment
approaches for metastatic renal cell carcinoma. Curr Oncol Rep
2000; 2(5) : 417-422.
-
Willis RA. The Spread of
Tumour in the Human Body. Butterworth and Co, London, 1952,
233-235.
|

